- Search Menu
- Sign in through your institution
- Advance articles
- Editor's Choice
- Supplements
- French Abstracts
- Portuguese Abstracts
- Spanish Abstracts
- Author Guidelines
- Submission Site
- Open Access
- About International Journal for Quality in Health Care
- About the International Society for Quality in Health Care
- Editorial Board
- Advertising and Corporate Services
- Journals Career Network
- Self-Archiving Policy
- Dispatch Dates
- Contact ISQua
- Journals on Oxford Academic
- Books on Oxford Academic


Article Contents
Primacy of the research question, structure of the paper, writing a research article: advice to beginners.
- Article contents
- Figures & tables
- Supplementary Data
Thomas V. Perneger, Patricia M. Hudelson, Writing a research article: advice to beginners, International Journal for Quality in Health Care , Volume 16, Issue 3, June 2004, Pages 191–192, https://doi.org/10.1093/intqhc/mzh053
- Permissions Icon Permissions
Writing research papers does not come naturally to most of us. The typical research paper is a highly codified rhetorical form [ 1 , 2 ]. Knowledge of the rules—some explicit, others implied—goes a long way toward writing a paper that will get accepted in a peer-reviewed journal.
A good research paper addresses a specific research question. The research question—or study objective or main research hypothesis—is the central organizing principle of the paper. Whatever relates to the research question belongs in the paper; the rest doesn’t. This is perhaps obvious when the paper reports on a well planned research project. However, in applied domains such as quality improvement, some papers are written based on projects that were undertaken for operational reasons, and not with the primary aim of producing new knowledge. In such cases, authors should define the main research question a posteriori and design the paper around it.
Generally, only one main research question should be addressed in a paper (secondary but related questions are allowed). If a project allows you to explore several distinct research questions, write several papers. For instance, if you measured the impact of obtaining written consent on patient satisfaction at a specialized clinic using a newly developed questionnaire, you may want to write one paper on the questionnaire development and validation, and another on the impact of the intervention. The idea is not to split results into ‘least publishable units’, a practice that is rightly decried, but rather into ‘optimally publishable units’.
What is a good research question? The key attributes are: (i) specificity; (ii) originality or novelty; and (iii) general relevance to a broad scientific community. The research question should be precise and not merely identify a general area of inquiry. It can often (but not always) be expressed in terms of a possible association between X and Y in a population Z, for example ‘we examined whether providing patients about to be discharged from the hospital with written information about their medications would improve their compliance with the treatment 1 month later’. A study does not necessarily have to break completely new ground, but it should extend previous knowledge in a useful way, or alternatively refute existing knowledge. Finally, the question should be of interest to others who work in the same scientific area. The latter requirement is more challenging for those who work in applied science than for basic scientists. While it may safely be assumed that the human genome is the same worldwide, whether the results of a local quality improvement project have wider relevance requires careful consideration and argument.
Once the research question is clearly defined, writing the paper becomes considerably easier. The paper will ask the question, then answer it. The key to successful scientific writing is getting the structure of the paper right. The basic structure of a typical research paper is the sequence of Introduction, Methods, Results, and Discussion (sometimes abbreviated as IMRAD). Each section addresses a different objective. The authors state: (i) the problem they intend to address—in other terms, the research question—in the Introduction; (ii) what they did to answer the question in the Methods section; (iii) what they observed in the Results section; and (iv) what they think the results mean in the Discussion.
In turn, each basic section addresses several topics, and may be divided into subsections (Table 1 ). In the Introduction, the authors should explain the rationale and background to the study. What is the research question, and why is it important to ask it? While it is neither necessary nor desirable to provide a full-blown review of the literature as a prelude to the study, it is helpful to situate the study within some larger field of enquiry. The research question should always be spelled out, and not merely left for the reader to guess.
Typical structure of a research paper
| Introduction |
| State why the problem you address is important |
| State what is lacking in the current knowledge |
| State the objectives of your study or the research question |
| Methods |
| Describe the context and setting of the study |
| Specify the study design |
| Describe the ‘population’ (patients, doctors, hospitals, etc.) |
| Describe the sampling strategy |
| Describe the intervention (if applicable) |
| Identify the main study variables |
| Describe data collection instruments and procedures |
| Outline analysis methods |
| Results |
| Report on data collection and recruitment (response rates, etc.) |
| Describe participants (demographic, clinical condition, etc.) |
| Present key findings with respect to the central research question |
| Present secondary findings (secondary outcomes, subgroup analyses, etc.) |
| Discussion |
| State the main findings of the study |
| Discuss the main results with reference to previous research |
| Discuss policy and practice implications of the results |
| Analyse the strengths and limitations of the study |
| Offer perspectives for future work |
| Introduction |
| State why the problem you address is important |
| State what is lacking in the current knowledge |
| State the objectives of your study or the research question |
| Methods |
| Describe the context and setting of the study |
| Specify the study design |
| Describe the ‘population’ (patients, doctors, hospitals, etc.) |
| Describe the sampling strategy |
| Describe the intervention (if applicable) |
| Identify the main study variables |
| Describe data collection instruments and procedures |
| Outline analysis methods |
| Results |
| Report on data collection and recruitment (response rates, etc.) |
| Describe participants (demographic, clinical condition, etc.) |
| Present key findings with respect to the central research question |
| Present secondary findings (secondary outcomes, subgroup analyses, etc.) |
| Discussion |
| State the main findings of the study |
| Discuss the main results with reference to previous research |
| Discuss policy and practice implications of the results |
| Analyse the strengths and limitations of the study |
| Offer perspectives for future work |
The Methods section should provide the readers with sufficient detail about the study methods to be able to reproduce the study if so desired. Thus, this section should be specific, concrete, technical, and fairly detailed. The study setting, the sampling strategy used, instruments, data collection methods, and analysis strategies should be described. In the case of qualitative research studies, it is also useful to tell the reader which research tradition the study utilizes and to link the choice of methodological strategies with the research goals [ 3 ].
The Results section is typically fairly straightforward and factual. All results that relate to the research question should be given in detail, including simple counts and percentages. Resist the temptation to demonstrate analytic ability and the richness of the dataset by providing numerous tables of non-essential results.
The Discussion section allows the most freedom. This is why the Discussion is the most difficult to write, and is often the weakest part of a paper. Structured Discussion sections have been proposed by some journal editors [ 4 ]. While strict adherence to such rules may not be necessary, following a plan such as that proposed in Table 1 may help the novice writer stay on track.
References should be used wisely. Key assertions should be referenced, as well as the methods and instruments used. However, unless the paper is a comprehensive review of a topic, there is no need to be exhaustive. Also, references to unpublished work, to documents in the grey literature (technical reports), or to any source that the reader will have difficulty finding or understanding should be avoided.
Having the structure of the paper in place is a good start. However, there are many details that have to be attended to while writing. An obvious recommendation is to read, and follow, the instructions to authors published by the journal (typically found on the journal’s website). Another concerns non-native writers of English: do have a native speaker edit the manuscript. A paper usually goes through several drafts before it is submitted. When revising a paper, it is useful to keep an eye out for the most common mistakes (Table 2 ). If you avoid all those, your paper should be in good shape.
Common mistakes seen in manuscripts submitted to this journal
| The research question is not specified |
| The stated aim of the paper is tautological (e.g. ‘The aim of this paper is to describe what we did’) or vague (e.g. ‘We explored issues related to X’) |
| The structure of the paper is chaotic (e.g. methods are described in the Results section) |
| The manuscripts does not follow the journal’s instructions for authors |
| The paper much exceeds the maximum number of words allowed |
| The Introduction is an extensive review of the literature |
| Methods, interventions and instruments are not described in sufficient detail |
| Results are reported selectively (e.g. percentages without frequencies, -values without measures of effect) |
| The same results appear both in a table and in the text |
| Detailed tables are provided for results that do not relate to the main research question |
| In the Introduction and Discussion, key arguments are not backed up by appropriate references |
| References are out of date or cannot be accessed by most readers |
| The Discussion does not provide an answer to the research question |
| The Discussion overstates the implications of the results and does not acknowledge the limitations of the study |
| The paper is written in poor English |
| The research question is not specified |
| The stated aim of the paper is tautological (e.g. ‘The aim of this paper is to describe what we did’) or vague (e.g. ‘We explored issues related to X’) |
| The structure of the paper is chaotic (e.g. methods are described in the Results section) |
| The manuscripts does not follow the journal’s instructions for authors |
| The paper much exceeds the maximum number of words allowed |
| The Introduction is an extensive review of the literature |
| Methods, interventions and instruments are not described in sufficient detail |
| Results are reported selectively (e.g. percentages without frequencies, -values without measures of effect) |
| The same results appear both in a table and in the text |
| Detailed tables are provided for results that do not relate to the main research question |
| In the Introduction and Discussion, key arguments are not backed up by appropriate references |
| References are out of date or cannot be accessed by most readers |
| The Discussion does not provide an answer to the research question |
| The Discussion overstates the implications of the results and does not acknowledge the limitations of the study |
| The paper is written in poor English |
Huth EJ . How to Write and Publish Papers in the Medical Sciences , 2nd edition. Baltimore, MD: Williams & Wilkins, 1990 .
Browner WS . Publishing and Presenting Clinical Research . Baltimore, MD: Lippincott, Williams & Wilkins, 1999 .
Devers KJ , Frankel RM. Getting qualitative research published. Educ Health 2001 ; 14 : 109 –117.
Docherty M , Smith R. The case for structuring the discussion of scientific papers. Br Med J 1999 ; 318 : 1224 –1225.
| Month: | Total Views: |
|---|---|
| December 2016 | 1 |
| January 2017 | 242 |
| February 2017 | 451 |
| March 2017 | 632 |
| April 2017 | 289 |
| May 2017 | 349 |
| June 2017 | 347 |
| July 2017 | 752 |
| August 2017 | 649 |
| September 2017 | 844 |
| October 2017 | 920 |
| November 2017 | 1,646 |
| December 2017 | 7,530 |
| January 2018 | 8,339 |
| February 2018 | 9,141 |
| March 2018 | 13,810 |
| April 2018 | 19,070 |
| May 2018 | 16,599 |
| June 2018 | 13,752 |
| July 2018 | 12,558 |
| August 2018 | 15,395 |
| September 2018 | 14,283 |
| October 2018 | 14,089 |
| November 2018 | 17,418 |
| December 2018 | 16,718 |
| January 2019 | 17,941 |
| February 2019 | 15,452 |
| March 2019 | 17,862 |
| April 2019 | 18,214 |
| May 2019 | 17,643 |
| June 2019 | 13,983 |
| July 2019 | 13,079 |
| August 2019 | 12,840 |
| September 2019 | 12,724 |
| October 2019 | 10,555 |
| November 2019 | 9,256 |
| December 2019 | 7,084 |
| January 2020 | 7,476 |
| February 2020 | 8,890 |
| March 2020 | 8,359 |
| April 2020 | 13,466 |
| May 2020 | 6,115 |
| June 2020 | 8,233 |
| July 2020 | 7,063 |
| August 2020 | 6,487 |
| September 2020 | 8,284 |
| October 2020 | 9,266 |
| November 2020 | 10,248 |
| December 2020 | 10,201 |
| January 2021 | 9,786 |
| February 2021 | 10,582 |
| March 2021 | 10,011 |
| April 2021 | 10,238 |
| May 2021 | 9,880 |
| June 2021 | 8,729 |
| July 2021 | 6,278 |
| August 2021 | 6,723 |
| September 2021 | 7,704 |
| October 2021 | 8,604 |
| November 2021 | 9,733 |
| December 2021 | 7,678 |
| January 2022 | 7,286 |
| February 2022 | 7,406 |
| March 2022 | 8,097 |
| April 2022 | 7,589 |
| May 2022 | 8,337 |
| June 2022 | 5,305 |
| July 2022 | 3,959 |
| August 2022 | 4,166 |
| September 2022 | 5,435 |
| October 2022 | 5,294 |
| November 2022 | 5,096 |
| December 2022 | 4,104 |
| January 2023 | 3,550 |
| February 2023 | 4,079 |
| March 2023 | 4,935 |
| April 2023 | 3,793 |
| May 2023 | 3,689 |
| June 2023 | 2,548 |
| July 2023 | 2,313 |
| August 2023 | 2,125 |
| September 2023 | 2,172 |
| October 2023 | 2,859 |
| November 2023 | 2,767 |
| December 2023 | 2,335 |
| January 2024 | 2,825 |
| February 2024 | 2,630 |
| March 2024 | 2,874 |
| April 2024 | 2,311 |
| May 2024 | 2,108 |
| June 2024 | 1,586 |
| July 2024 | 8,045 |
| August 2024 | 1,924 |
Email alerts
Citing articles via.
- Recommend to your Library
Affiliations
- Online ISSN 1464-3677
- Print ISSN 1353-4505
- Copyright © 2024 International Society for Quality in Health Care and Oxford University Press
- About Oxford Academic
- Publish journals with us
- University press partners
- What we publish
- New features
- Open access
- Institutional account management
- Rights and permissions
- Get help with access
- Accessibility
- Advertising
- Media enquiries
- Oxford University Press
- Oxford Languages
- University of Oxford
Oxford University Press is a department of the University of Oxford. It furthers the University's objective of excellence in research, scholarship, and education by publishing worldwide
- Copyright © 2024 Oxford University Press
- Cookie settings
- Cookie policy
- Privacy policy
- Legal notice
This Feature Is Available To Subscribers Only
Sign In or Create an Account
This PDF is available to Subscribers Only
For full access to this pdf, sign in to an existing account, or purchase an annual subscription.
Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
13.1 Formatting a Research Paper
Learning objectives.
- Identify the major components of a research paper written using American Psychological Association (APA) style.
- Apply general APA style and formatting conventions in a research paper.
In this chapter, you will learn how to use APA style , the documentation and formatting style followed by the American Psychological Association, as well as MLA style , from the Modern Language Association. There are a few major formatting styles used in academic texts, including AMA, Chicago, and Turabian:
- AMA (American Medical Association) for medicine, health, and biological sciences
- APA (American Psychological Association) for education, psychology, and the social sciences
- Chicago—a common style used in everyday publications like magazines, newspapers, and books
- MLA (Modern Language Association) for English, literature, arts, and humanities
- Turabian—another common style designed for its universal application across all subjects and disciplines
While all the formatting and citation styles have their own use and applications, in this chapter we focus our attention on the two styles you are most likely to use in your academic studies: APA and MLA.
If you find that the rules of proper source documentation are difficult to keep straight, you are not alone. Writing a good research paper is, in and of itself, a major intellectual challenge. Having to follow detailed citation and formatting guidelines as well may seem like just one more task to add to an already-too-long list of requirements.
Following these guidelines, however, serves several important purposes. First, it signals to your readers that your paper should be taken seriously as a student’s contribution to a given academic or professional field; it is the literary equivalent of wearing a tailored suit to a job interview. Second, it shows that you respect other people’s work enough to give them proper credit for it. Finally, it helps your reader find additional materials if he or she wishes to learn more about your topic.
Furthermore, producing a letter-perfect APA-style paper need not be burdensome. Yes, it requires careful attention to detail. However, you can simplify the process if you keep these broad guidelines in mind:
- Work ahead whenever you can. Chapter 11 “Writing from Research: What Will I Learn?” includes tips for keeping track of your sources early in the research process, which will save time later on.
- Get it right the first time. Apply APA guidelines as you write, so you will not have much to correct during the editing stage. Again, putting in a little extra time early on can save time later.
- Use the resources available to you. In addition to the guidelines provided in this chapter, you may wish to consult the APA website at http://www.apa.org or the Purdue University Online Writing lab at http://owl.english.purdue.edu , which regularly updates its online style guidelines.
General Formatting Guidelines
This chapter provides detailed guidelines for using the citation and formatting conventions developed by the American Psychological Association, or APA. Writers in disciplines as diverse as astrophysics, biology, psychology, and education follow APA style. The major components of a paper written in APA style are listed in the following box.
These are the major components of an APA-style paper:
Body, which includes the following:
- Headings and, if necessary, subheadings to organize the content
- In-text citations of research sources
- References page
All these components must be saved in one document, not as separate documents.
The title page of your paper includes the following information:
- Title of the paper
- Author’s name
- Name of the institution with which the author is affiliated
- Header at the top of the page with the paper title (in capital letters) and the page number (If the title is lengthy, you may use a shortened form of it in the header.)
List the first three elements in the order given in the previous list, centered about one third of the way down from the top of the page. Use the headers and footers tool of your word-processing program to add the header, with the title text at the left and the page number in the upper-right corner. Your title page should look like the following example.

The next page of your paper provides an abstract , or brief summary of your findings. An abstract does not need to be provided in every paper, but an abstract should be used in papers that include a hypothesis. A good abstract is concise—about one hundred fifty to two hundred fifty words—and is written in an objective, impersonal style. Your writing voice will not be as apparent here as in the body of your paper. When writing the abstract, take a just-the-facts approach, and summarize your research question and your findings in a few sentences.
In Chapter 12 “Writing a Research Paper” , you read a paper written by a student named Jorge, who researched the effectiveness of low-carbohydrate diets. Read Jorge’s abstract. Note how it sums up the major ideas in his paper without going into excessive detail.

Write an abstract summarizing your paper. Briefly introduce the topic, state your findings, and sum up what conclusions you can draw from your research. Use the word count feature of your word-processing program to make sure your abstract does not exceed one hundred fifty words.
Depending on your field of study, you may sometimes write research papers that present extensive primary research, such as your own experiment or survey. In your abstract, summarize your research question and your findings, and briefly indicate how your study relates to prior research in the field.
Margins, Pagination, and Headings
APA style requirements also address specific formatting concerns, such as margins, pagination, and heading styles, within the body of the paper. Review the following APA guidelines.
Use these general guidelines to format the paper:
- Set the top, bottom, and side margins of your paper at 1 inch.
- Use double-spaced text throughout your paper.
- Use a standard font, such as Times New Roman or Arial, in a legible size (10- to 12-point).
- Use continuous pagination throughout the paper, including the title page and the references section. Page numbers appear flush right within your header.
- Section headings and subsection headings within the body of your paper use different types of formatting depending on the level of information you are presenting. Additional details from Jorge’s paper are provided.

Begin formatting the final draft of your paper according to APA guidelines. You may work with an existing document or set up a new document if you choose. Include the following:
- Your title page
- The abstract you created in Note 13.8 “Exercise 1”
- Correct headers and page numbers for your title page and abstract
APA style uses section headings to organize information, making it easy for the reader to follow the writer’s train of thought and to know immediately what major topics are covered. Depending on the length and complexity of the paper, its major sections may also be divided into subsections, sub-subsections, and so on. These smaller sections, in turn, use different heading styles to indicate different levels of information. In essence, you are using headings to create a hierarchy of information.
The following heading styles used in APA formatting are listed in order of greatest to least importance:
- Section headings use centered, boldface type. Headings use title case, with important words in the heading capitalized.
- Subsection headings use left-aligned, boldface type. Headings use title case.
- The third level uses left-aligned, indented, boldface type. Headings use a capital letter only for the first word, and they end in a period.
- The fourth level follows the same style used for the previous level, but the headings are boldfaced and italicized.
- The fifth level follows the same style used for the previous level, but the headings are italicized and not boldfaced.
Visually, the hierarchy of information is organized as indicated in Table 13.1 “Section Headings” .
Table 13.1 Section Headings
| Level of Information | Text Example |
|---|---|
| Level 1 | |
| Level 2 | |
| Level 3 | |
| Level 4 | |
| Level 5 |
A college research paper may not use all the heading levels shown in Table 13.1 “Section Headings” , but you are likely to encounter them in academic journal articles that use APA style. For a brief paper, you may find that level 1 headings suffice. Longer or more complex papers may need level 2 headings or other lower-level headings to organize information clearly. Use your outline to craft your major section headings and determine whether any subtopics are substantial enough to require additional levels of headings.
Working with the document you developed in Note 13.11 “Exercise 2” , begin setting up the heading structure of the final draft of your research paper according to APA guidelines. Include your title and at least two to three major section headings, and follow the formatting guidelines provided above. If your major sections should be broken into subsections, add those headings as well. Use your outline to help you.
Because Jorge used only level 1 headings, his Exercise 3 would look like the following:
| Level of Information | Text Example |
|---|---|
| Level 1 | |
| Level 1 | |
| Level 1 | |
| Level 1 |
Citation Guidelines
In-text citations.
Throughout the body of your paper, include a citation whenever you quote or paraphrase material from your research sources. As you learned in Chapter 11 “Writing from Research: What Will I Learn?” , the purpose of citations is twofold: to give credit to others for their ideas and to allow your reader to follow up and learn more about the topic if desired. Your in-text citations provide basic information about your source; each source you cite will have a longer entry in the references section that provides more detailed information.
In-text citations must provide the name of the author or authors and the year the source was published. (When a given source does not list an individual author, you may provide the source title or the name of the organization that published the material instead.) When directly quoting a source, it is also required that you include the page number where the quote appears in your citation.
This information may be included within the sentence or in a parenthetical reference at the end of the sentence, as in these examples.
Epstein (2010) points out that “junk food cannot be considered addictive in the same way that we think of psychoactive drugs as addictive” (p. 137).
Here, the writer names the source author when introducing the quote and provides the publication date in parentheses after the author’s name. The page number appears in parentheses after the closing quotation marks and before the period that ends the sentence.
Addiction researchers caution that “junk food cannot be considered addictive in the same way that we think of psychoactive drugs as addictive” (Epstein, 2010, p. 137).
Here, the writer provides a parenthetical citation at the end of the sentence that includes the author’s name, the year of publication, and the page number separated by commas. Again, the parenthetical citation is placed after the closing quotation marks and before the period at the end of the sentence.
As noted in the book Junk Food, Junk Science (Epstein, 2010, p. 137), “junk food cannot be considered addictive in the same way that we think of psychoactive drugs as addictive.”
Here, the writer chose to mention the source title in the sentence (an optional piece of information to include) and followed the title with a parenthetical citation. Note that the parenthetical citation is placed before the comma that signals the end of the introductory phrase.
David Epstein’s book Junk Food, Junk Science (2010) pointed out that “junk food cannot be considered addictive in the same way that we think of psychoactive drugs as addictive” (p. 137).
Another variation is to introduce the author and the source title in your sentence and include the publication date and page number in parentheses within the sentence or at the end of the sentence. As long as you have included the essential information, you can choose the option that works best for that particular sentence and source.
Citing a book with a single author is usually a straightforward task. Of course, your research may require that you cite many other types of sources, such as books or articles with more than one author or sources with no individual author listed. You may also need to cite sources available in both print and online and nonprint sources, such as websites and personal interviews. Chapter 13 “APA and MLA Documentation and Formatting” , Section 13.2 “Citing and Referencing Techniques” and Section 13.3 “Creating a References Section” provide extensive guidelines for citing a variety of source types.
Writing at Work
APA is just one of several different styles with its own guidelines for documentation, formatting, and language usage. Depending on your field of interest, you may be exposed to additional styles, such as the following:
- MLA style. Determined by the Modern Languages Association and used for papers in literature, languages, and other disciplines in the humanities.
- Chicago style. Outlined in the Chicago Manual of Style and sometimes used for papers in the humanities and the sciences; many professional organizations use this style for publications as well.
- Associated Press (AP) style. Used by professional journalists.
References List
The brief citations included in the body of your paper correspond to the more detailed citations provided at the end of the paper in the references section. In-text citations provide basic information—the author’s name, the publication date, and the page number if necessary—while the references section provides more extensive bibliographical information. Again, this information allows your reader to follow up on the sources you cited and do additional reading about the topic if desired.
The specific format of entries in the list of references varies slightly for different source types, but the entries generally include the following information:
- The name(s) of the author(s) or institution that wrote the source
- The year of publication and, where applicable, the exact date of publication
- The full title of the source
- For books, the city of publication
- For articles or essays, the name of the periodical or book in which the article or essay appears
- For magazine and journal articles, the volume number, issue number, and pages where the article appears
- For sources on the web, the URL where the source is located
The references page is double spaced and lists entries in alphabetical order by the author’s last name. If an entry continues for more than one line, the second line and each subsequent line are indented five spaces. Review the following example. ( Chapter 13 “APA and MLA Documentation and Formatting” , Section 13.3 “Creating a References Section” provides extensive guidelines for formatting reference entries for different types of sources.)

In APA style, book and article titles are formatted in sentence case, not title case. Sentence case means that only the first word is capitalized, along with any proper nouns.
Key Takeaways
- Following proper citation and formatting guidelines helps writers ensure that their work will be taken seriously, give proper credit to other authors for their work, and provide valuable information to readers.
- Working ahead and taking care to cite sources correctly the first time are ways writers can save time during the editing stage of writing a research paper.
- APA papers usually include an abstract that concisely summarizes the paper.
- APA papers use a specific headings structure to provide a clear hierarchy of information.
- In APA papers, in-text citations usually include the name(s) of the author(s) and the year of publication.
- In-text citations correspond to entries in the references section, which provide detailed bibliographical information about a source.
Writing for Success Copyright © 2015 by University of Minnesota is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License , except where otherwise noted.
- Privacy Policy
Home » Research Paper Format – Types, Examples and Templates
Research Paper Format – Types, Examples and Templates
Table of Contents

Research paper format is an essential aspect of academic writing that plays a crucial role in the communication of research findings . The format of a research paper depends on various factors such as the discipline, style guide, and purpose of the research. It includes guidelines for the structure, citation style, referencing , and other elements of the paper that contribute to its overall presentation and coherence. Adhering to the appropriate research paper format is vital for ensuring that the research is accurately and effectively communicated to the intended audience. In this era of information, it is essential to understand the different research paper formats and their guidelines to communicate research effectively, accurately, and with the required level of detail. This post aims to provide an overview of some of the common research paper formats used in academic writing.
Research Paper Formats
Research Paper Formats are as follows:
- APA (American Psychological Association) format
- MLA (Modern Language Association) format
- Chicago/Turabian style
- IEEE (Institute of Electrical and Electronics Engineers) format
- AMA (American Medical Association) style
- Harvard style
- Vancouver style
- ACS (American Chemical Society) style
- ASA (American Sociological Association) style
- APSA (American Political Science Association) style
APA (American Psychological Association) Format
Here is a general APA format for a research paper:
- Title Page: The title page should include the title of your paper, your name, and your institutional affiliation. It should also include a running head, which is a shortened version of the title, and a page number in the upper right-hand corner.
- Abstract : The abstract is a brief summary of your paper, typically 150-250 words. It should include the purpose of your research, the main findings, and any implications or conclusions that can be drawn.
- Introduction: The introduction should provide background information on your topic, state the purpose of your research, and present your research question or hypothesis. It should also include a brief literature review that discusses previous research on your topic.
- Methods: The methods section should describe the procedures you used to collect and analyze your data. It should include information on the participants, the materials and instruments used, and the statistical analyses performed.
- Results: The results section should present the findings of your research in a clear and concise manner. Use tables and figures to help illustrate your results.
- Discussion : The discussion section should interpret your results and relate them back to your research question or hypothesis. It should also discuss the implications of your findings and any limitations of your study.
- References : The references section should include a list of all sources cited in your paper. Follow APA formatting guidelines for your citations and references.
Some additional tips for formatting your APA research paper:
- Use 12-point Times New Roman font throughout the paper.
- Double-space all text, including the references.
- Use 1-inch margins on all sides of the page.
- Indent the first line of each paragraph by 0.5 inches.
- Use a hanging indent for the references (the first line should be flush with the left margin, and all subsequent lines should be indented).
- Number all pages, including the title page and references page, in the upper right-hand corner.
APA Research Paper Format Template
APA Research Paper Format Template is as follows:
Title Page:
- Title of the paper
- Author’s name
- Institutional affiliation
- A brief summary of the main points of the paper, including the research question, methods, findings, and conclusions. The abstract should be no more than 250 words.
Introduction:
- Background information on the topic of the research paper
- Research question or hypothesis
- Significance of the study
- Overview of the research methods and design
- Brief summary of the main findings
- Participants: description of the sample population, including the number of participants and their characteristics (age, gender, ethnicity, etc.)
- Materials: description of any materials used in the study (e.g., survey questions, experimental apparatus)
- Procedure: detailed description of the steps taken to conduct the study
- Presentation of the findings of the study, including statistical analyses if applicable
- Tables and figures may be included to illustrate the results
Discussion:
- Interpretation of the results in light of the research question and hypothesis
- Implications of the study for the field
- Limitations of the study
- Suggestions for future research
References:
- A list of all sources cited in the paper, in APA format
Formatting guidelines:
- Double-spaced
- 12-point font (Times New Roman or Arial)
- 1-inch margins on all sides
- Page numbers in the top right corner
- Headings and subheadings should be used to organize the paper
- The first line of each paragraph should be indented
- Quotations of 40 or more words should be set off in a block quote with no quotation marks
- In-text citations should include the author’s last name and year of publication (e.g., Smith, 2019)
APA Research Paper Format Example
APA Research Paper Format Example is as follows:
The Effects of Social Media on Mental Health
University of XYZ
This study examines the relationship between social media use and mental health among college students. Data was collected through a survey of 500 students at the University of XYZ. Results suggest that social media use is significantly related to symptoms of depression and anxiety, and that the negative effects of social media are greater among frequent users.
Social media has become an increasingly important aspect of modern life, especially among young adults. While social media can have many positive effects, such as connecting people across distances and sharing information, there is growing concern about its impact on mental health. This study aims to examine the relationship between social media use and mental health among college students.
Participants: Participants were 500 college students at the University of XYZ, recruited through online advertisements and flyers posted on campus. Participants ranged in age from 18 to 25, with a mean age of 20.5 years. The sample was 60% female, 40% male, and 5% identified as non-binary or gender non-conforming.
Data was collected through an online survey administered through Qualtrics. The survey consisted of several measures, including the Patient Health Questionnaire-9 (PHQ-9) for depression symptoms, the Generalized Anxiety Disorder-7 (GAD-7) for anxiety symptoms, and questions about social media use.
Procedure :
Participants were asked to complete the online survey at their convenience. The survey took approximately 20-30 minutes to complete. Data was analyzed using descriptive statistics, correlations, and multiple regression analysis.
Results indicated that social media use was significantly related to symptoms of depression (r = .32, p < .001) and anxiety (r = .29, p < .001). Regression analysis indicated that frequency of social media use was a significant predictor of both depression symptoms (β = .24, p < .001) and anxiety symptoms (β = .20, p < .001), even when controlling for age, gender, and other relevant factors.
The results of this study suggest that social media use is associated with symptoms of depression and anxiety among college students. The negative effects of social media are greater among frequent users. These findings have important implications for mental health professionals and educators, who should consider addressing the potential negative effects of social media use in their work with young adults.
References :
References should be listed in alphabetical order according to the author’s last name. For example:
- Chou, H. T. G., & Edge, N. (2012). “They are happier and having better lives than I am”: The impact of using Facebook on perceptions of others’ lives. Cyberpsychology, Behavior, and Social Networking, 15(2), 117-121.
- Twenge, J. M., Joiner, T. E., Rogers, M. L., & Martin, G. N. (2018). Increases in depressive symptoms, suicide-related outcomes, and suicide rates among U.S. adolescents after 2010 and links to increased new media screen time. Clinical Psychological Science, 6(1), 3-17.
Note: This is just a sample Example do not use this in your assignment.
MLA (Modern Language Association) Format
MLA (Modern Language Association) Format is as follows:
- Page Layout : Use 8.5 x 11-inch white paper, with 1-inch margins on all sides. The font should be 12-point Times New Roman or a similar serif font.
- Heading and Title : The first page of your research paper should include a heading and a title. The heading should include your name, your instructor’s name, the course title, and the date. The title should be centered and in title case (capitalizing the first letter of each important word).
- In-Text Citations : Use parenthetical citations to indicate the source of your information. The citation should include the author’s last name and the page number(s) of the source. For example: (Smith 23).
- Works Cited Page : At the end of your paper, include a Works Cited page that lists all the sources you used in your research. Each entry should include the author’s name, the title of the work, the publication information, and the medium of publication.
- Formatting Quotations : Use double quotation marks for short quotations and block quotations for longer quotations. Indent the entire quotation five spaces from the left margin.
- Formatting the Body : Use a clear and readable font and double-space your text throughout. The first line of each paragraph should be indented one-half inch from the left margin.
MLA Research Paper Template
MLA Research Paper Format Template is as follows:
- Use 8.5 x 11 inch white paper.
- Use a 12-point font, such as Times New Roman.
- Use double-spacing throughout the entire paper, including the title page and works cited page.
- Set the margins to 1 inch on all sides.
- Use page numbers in the upper right corner, beginning with the first page of text.
- Include a centered title for the research paper, using title case (capitalizing the first letter of each important word).
- Include your name, instructor’s name, course name, and date in the upper left corner, double-spaced.
In-Text Citations
- When quoting or paraphrasing information from sources, include an in-text citation within the text of your paper.
- Use the author’s last name and the page number in parentheses at the end of the sentence, before the punctuation mark.
- If the author’s name is mentioned in the sentence, only include the page number in parentheses.
Works Cited Page
- List all sources cited in alphabetical order by the author’s last name.
- Each entry should include the author’s name, title of the work, publication information, and medium of publication.
- Use italics for book and journal titles, and quotation marks for article and chapter titles.
- For online sources, include the date of access and the URL.
Here is an example of how the first page of a research paper in MLA format should look:
Headings and Subheadings
- Use headings and subheadings to organize your paper and make it easier to read.
- Use numerals to number your headings and subheadings (e.g. 1, 2, 3), and capitalize the first letter of each word.
- The main heading should be centered and in boldface type, while subheadings should be left-aligned and in italics.
- Use only one space after each period or punctuation mark.
- Use quotation marks to indicate direct quotes from a source.
- If the quote is more than four lines, format it as a block quote, indented one inch from the left margin and without quotation marks.
- Use ellipses (…) to indicate omitted words from a quote, and brackets ([…]) to indicate added words.
Works Cited Examples
- Book: Last Name, First Name. Title of Book. Publisher, Publication Year.
- Journal Article: Last Name, First Name. “Title of Article.” Title of Journal, volume number, issue number, publication date, page numbers.
- Website: Last Name, First Name. “Title of Webpage.” Title of Website, publication date, URL. Accessed date.
Here is an example of how a works cited entry for a book should look:
Smith, John. The Art of Writing Research Papers. Penguin, 2021.
MLA Research Paper Example
MLA Research Paper Format Example is as follows:
Your Professor’s Name
Course Name and Number
Date (in Day Month Year format)
Word Count (not including title page or Works Cited)
Title: The Impact of Video Games on Aggression Levels
Video games have become a popular form of entertainment among people of all ages. However, the impact of video games on aggression levels has been a subject of debate among scholars and researchers. While some argue that video games promote aggression and violent behavior, others argue that there is no clear link between video games and aggression levels. This research paper aims to explore the impact of video games on aggression levels among young adults.
Background:
The debate on the impact of video games on aggression levels has been ongoing for several years. According to the American Psychological Association, exposure to violent media, including video games, can increase aggression levels in children and adolescents. However, some researchers argue that there is no clear evidence to support this claim. Several studies have been conducted to examine the impact of video games on aggression levels, but the results have been mixed.
Methodology:
This research paper used a quantitative research approach to examine the impact of video games on aggression levels among young adults. A sample of 100 young adults between the ages of 18 and 25 was selected for the study. The participants were asked to complete a questionnaire that measured their aggression levels and their video game habits.
The results of the study showed that there was a significant correlation between video game habits and aggression levels among young adults. The participants who reported playing violent video games for more than 5 hours per week had higher aggression levels than those who played less than 5 hours per week. The study also found that male participants were more likely to play violent video games and had higher aggression levels than female participants.
The findings of this study support the claim that video games can increase aggression levels among young adults. However, it is important to note that the study only examined the impact of video games on aggression levels and did not take into account other factors that may contribute to aggressive behavior. It is also important to note that not all video games promote violence and aggression, and some games may have a positive impact on cognitive and social skills.
Conclusion :
In conclusion, this research paper provides evidence to support the claim that video games can increase aggression levels among young adults. However, it is important to conduct further research to examine the impact of video games on other aspects of behavior and to explore the potential benefits of video games. Parents and educators should be aware of the potential impact of video games on aggression levels and should encourage young adults to engage in a variety of activities that promote cognitive and social skills.
Works Cited:
- American Psychological Association. (2017). Violent Video Games: Myths, Facts, and Unanswered Questions. Retrieved from https://www.apa.org/news/press/releases/2017/08/violent-video-games
- Ferguson, C. J. (2015). Do Angry Birds make for angry children? A meta-analysis of video game influences on children’s and adolescents’ aggression, mental health, prosocial behavior, and academic performance. Perspectives on Psychological Science, 10(5), 646-666.
- Gentile, D. A., Swing, E. L., Lim, C. G., & Khoo, A. (2012). Video game playing, attention problems, and impulsiveness: Evidence of bidirectional causality. Psychology of Popular Media Culture, 1(1), 62-70.
- Greitemeyer, T. (2014). Effects of prosocial video games on prosocial behavior. Journal of Personality and Social Psychology, 106(4), 530-548.
Chicago/Turabian Style
Chicago/Turabian Formate is as follows:
- Margins : Use 1-inch margins on all sides of the paper.
- Font : Use a readable font such as Times New Roman or Arial, and use a 12-point font size.
- Page numbering : Number all pages in the upper right-hand corner, beginning with the first page of text. Use Arabic numerals.
- Title page: Include a title page with the title of the paper, your name, course title and number, instructor’s name, and the date. The title should be centered on the page and in title case (capitalize the first letter of each word).
- Headings: Use headings to organize your paper. The first level of headings should be centered and in boldface or italics. The second level of headings should be left-aligned and in boldface or italics. Use as many levels of headings as necessary to organize your paper.
- In-text citations : Use footnotes or endnotes to cite sources within the text of your paper. The first citation for each source should be a full citation, and subsequent citations can be shortened. Use superscript numbers to indicate footnotes or endnotes.
- Bibliography : Include a bibliography at the end of your paper, listing all sources cited in your paper. The bibliography should be in alphabetical order by the author’s last name, and each entry should include the author’s name, title of the work, publication information, and date of publication.
- Formatting of quotations: Use block quotations for quotations that are longer than four lines. Indent the entire quotation one inch from the left margin, and do not use quotation marks. Single-space the quotation, and double-space between paragraphs.
- Tables and figures: Use tables and figures to present data and illustrations. Number each table and figure sequentially, and provide a brief title for each. Place tables and figures as close as possible to the text that refers to them.
- Spelling and grammar : Use correct spelling and grammar throughout your paper. Proofread carefully for errors.
Chicago/Turabian Research Paper Template
Chicago/Turabian Research Paper Template is as folows:
Title of Paper
Name of Student
Professor’s Name
I. Introduction
A. Background Information
B. Research Question
C. Thesis Statement
II. Literature Review
A. Overview of Existing Literature
B. Analysis of Key Literature
C. Identification of Gaps in Literature
III. Methodology
A. Research Design
B. Data Collection
C. Data Analysis
IV. Results
A. Presentation of Findings
B. Analysis of Findings
C. Discussion of Implications
V. Conclusion
A. Summary of Findings
B. Implications for Future Research
C. Conclusion
VI. References
A. Bibliography
B. In-Text Citations
VII. Appendices (if necessary)
A. Data Tables
C. Additional Supporting Materials
Chicago/Turabian Research Paper Example
Title: The Impact of Social Media on Political Engagement
Name: John Smith
Class: POLS 101
Professor: Dr. Jane Doe
Date: April 8, 2023
I. Introduction:
Social media has become an integral part of our daily lives. People use social media platforms like Facebook, Twitter, and Instagram to connect with friends and family, share their opinions, and stay informed about current events. With the rise of social media, there has been a growing interest in understanding its impact on various aspects of society, including political engagement. In this paper, I will examine the relationship between social media use and political engagement, specifically focusing on how social media influences political participation and political attitudes.
II. Literature Review:
There is a growing body of literature on the impact of social media on political engagement. Some scholars argue that social media has a positive effect on political participation by providing new channels for political communication and mobilization (Delli Carpini & Keeter, 1996; Putnam, 2000). Others, however, suggest that social media can have a negative impact on political engagement by creating filter bubbles that reinforce existing beliefs and discourage political dialogue (Pariser, 2011; Sunstein, 2001).
III. Methodology:
To examine the relationship between social media use and political engagement, I conducted a survey of 500 college students. The survey included questions about social media use, political participation, and political attitudes. The data was analyzed using descriptive statistics and regression analysis.
Iv. Results:
The results of the survey indicate that social media use is positively associated with political participation. Specifically, respondents who reported using social media to discuss politics were more likely to have participated in a political campaign, attended a political rally, or contacted a political representative. Additionally, social media use was found to be associated with more positive attitudes towards political engagement, such as increased trust in government and belief in the effectiveness of political action.
V. Conclusion:
The findings of this study suggest that social media has a positive impact on political engagement, by providing new opportunities for political communication and mobilization. However, there is also a need for caution, as social media can also create filter bubbles that reinforce existing beliefs and discourage political dialogue. Future research should continue to explore the complex relationship between social media and political engagement, and develop strategies to harness the potential benefits of social media while mitigating its potential negative effects.
Vii. References:
- Delli Carpini, M. X., & Keeter, S. (1996). What Americans know about politics and why it matters. Yale University Press.
- Pariser, E. (2011). The filter bubble: What the Internet is hiding from you. Penguin.
- Putnam, R. D. (2000). Bowling alone: The collapse and revival of American community. Simon & Schuster.
- Sunstein, C. R. (2001). Republic.com. Princeton University Press.
IEEE (Institute of Electrical and Electronics Engineers) Format
IEEE (Institute of Electrical and Electronics Engineers) Research Paper Format is as follows:
- Title : A concise and informative title that accurately reflects the content of the paper.
- Abstract : A brief summary of the paper, typically no more than 250 words, that includes the purpose of the study, the methods used, the key findings, and the main conclusions.
- Introduction : An overview of the background, context, and motivation for the research, including a clear statement of the problem being addressed and the objectives of the study.
- Literature review: A critical analysis of the relevant research and scholarship on the topic, including a discussion of any gaps or limitations in the existing literature.
- Methodology : A detailed description of the methods used to collect and analyze data, including any experiments or simulations, data collection instruments or procedures, and statistical analyses.
- Results : A clear and concise presentation of the findings, including any relevant tables, graphs, or figures.
- Discussion : A detailed interpretation of the results, including a comparison of the findings with previous research, a discussion of the implications of the results, and any recommendations for future research.
- Conclusion : A summary of the key findings and main conclusions of the study.
- References : A list of all sources cited in the paper, formatted according to IEEE guidelines.
In addition to these elements, an IEEE research paper should also follow certain formatting guidelines, including using 12-point font, double-spaced text, and numbered headings and subheadings. Additionally, any tables, figures, or equations should be clearly labeled and referenced in the text.
AMA (American Medical Association) Style
AMA (American Medical Association) Style Research Paper Format:
- Title Page: This page includes the title of the paper, the author’s name, institutional affiliation, and any acknowledgments or disclaimers.
- Abstract: The abstract is a brief summary of the paper that outlines the purpose, methods, results, and conclusions of the study. It is typically limited to 250 words or less.
- Introduction: The introduction provides a background of the research problem, defines the research question, and outlines the objectives and hypotheses of the study.
- Methods: The methods section describes the research design, participants, procedures, and instruments used to collect and analyze data.
- Results: The results section presents the findings of the study in a clear and concise manner, using graphs, tables, and charts where appropriate.
- Discussion: The discussion section interprets the results, explains their significance, and relates them to previous research in the field.
- Conclusion: The conclusion summarizes the main points of the paper, discusses the implications of the findings, and suggests future research directions.
- References: The reference list includes all sources cited in the paper, listed in alphabetical order by author’s last name.
In addition to these sections, the AMA format requires that authors follow specific guidelines for citing sources in the text and formatting their references. The AMA style uses a superscript number system for in-text citations and provides specific formats for different types of sources, such as books, journal articles, and websites.
Harvard Style
Harvard Style Research Paper format is as follows:
- Title page: This should include the title of your paper, your name, the name of your institution, and the date of submission.
- Abstract : This is a brief summary of your paper, usually no more than 250 words. It should outline the main points of your research and highlight your findings.
- Introduction : This section should introduce your research topic, provide background information, and outline your research question or thesis statement.
- Literature review: This section should review the relevant literature on your topic, including previous research studies, academic articles, and other sources.
- Methodology : This section should describe the methods you used to conduct your research, including any data collection methods, research instruments, and sampling techniques.
- Results : This section should present your findings in a clear and concise manner, using tables, graphs, and other visual aids if necessary.
- Discussion : This section should interpret your findings and relate them to the broader research question or thesis statement. You should also discuss the implications of your research and suggest areas for future study.
- Conclusion : This section should summarize your main findings and provide a final statement on the significance of your research.
- References : This is a list of all the sources you cited in your paper, presented in alphabetical order by author name. Each citation should include the author’s name, the title of the source, the publication date, and other relevant information.
In addition to these sections, a Harvard Style research paper may also include a table of contents, appendices, and other supplementary materials as needed. It is important to follow the specific formatting guidelines provided by your instructor or academic institution when preparing your research paper in Harvard Style.
Vancouver Style
Vancouver Style Research Paper format is as follows:
The Vancouver citation style is commonly used in the biomedical sciences and is known for its use of numbered references. Here is a basic format for a research paper using the Vancouver citation style:
- Title page: Include the title of your paper, your name, the name of your institution, and the date.
- Abstract : This is a brief summary of your research paper, usually no more than 250 words.
- Introduction : Provide some background information on your topic and state the purpose of your research.
- Methods : Describe the methods you used to conduct your research, including the study design, data collection, and statistical analysis.
- Results : Present your findings in a clear and concise manner, using tables and figures as needed.
- Discussion : Interpret your results and explain their significance. Also, discuss any limitations of your study and suggest directions for future research.
- References : List all of the sources you cited in your paper in numerical order. Each reference should include the author’s name, the title of the article or book, the name of the journal or publisher, the year of publication, and the page numbers.
ACS (American Chemical Society) Style
ACS (American Chemical Society) Style Research Paper format is as follows:
The American Chemical Society (ACS) Style is a citation style commonly used in chemistry and related fields. When formatting a research paper in ACS Style, here are some guidelines to follow:
- Paper Size and Margins : Use standard 8.5″ x 11″ paper with 1-inch margins on all sides.
- Font: Use a 12-point serif font (such as Times New Roman) for the main text. The title should be in bold and a larger font size.
- Title Page : The title page should include the title of the paper, the authors’ names and affiliations, and the date of submission. The title should be centered on the page and written in bold font. The authors’ names should be centered below the title, followed by their affiliations and the date.
- Abstract : The abstract should be a brief summary of the paper, no more than 250 words. It should be on a separate page and include the title of the paper, the authors’ names and affiliations, and the text of the abstract.
- Main Text : The main text should be organized into sections with headings that clearly indicate the content of each section. The introduction should provide background information and state the research question or hypothesis. The methods section should describe the procedures used in the study. The results section should present the findings of the study, and the discussion section should interpret the results and provide conclusions.
- References: Use the ACS Style guide to format the references cited in the paper. In-text citations should be numbered sequentially throughout the text and listed in numerical order at the end of the paper.
- Figures and Tables: Figures and tables should be numbered sequentially and referenced in the text. Each should have a descriptive caption that explains its content. Figures should be submitted in a high-quality electronic format.
- Supporting Information: Additional information such as data, graphs, and videos may be included as supporting information. This should be included in a separate file and referenced in the main text.
- Acknowledgments : Acknowledge any funding sources or individuals who contributed to the research.
ASA (American Sociological Association) Style
ASA (American Sociological Association) Style Research Paper format is as follows:
- Title Page: The title page of an ASA style research paper should include the title of the paper, the author’s name, and the institutional affiliation. The title should be centered and should be in title case (the first letter of each major word should be capitalized).
- Abstract: An abstract is a brief summary of the paper that should appear on a separate page immediately following the title page. The abstract should be no more than 200 words in length and should summarize the main points of the paper.
- Main Body: The main body of the paper should begin on a new page following the abstract page. The paper should be double-spaced, with 1-inch margins on all sides, and should be written in 12-point Times New Roman font. The main body of the paper should include an introduction, a literature review, a methodology section, results, and a discussion.
- References : The reference section should appear on a separate page at the end of the paper. All sources cited in the paper should be listed in alphabetical order by the author’s last name. Each reference should include the author’s name, the title of the work, the publication information, and the date of publication.
- Appendices : Appendices are optional and should only be included if they contain information that is relevant to the study but too lengthy to be included in the main body of the paper. If you include appendices, each one should be labeled with a letter (e.g., Appendix A, Appendix B, etc.) and should be referenced in the main body of the paper.
APSA (American Political Science Association) Style
APSA (American Political Science Association) Style Research Paper format is as follows:
- Title Page: The title page should include the title of the paper, the author’s name, the name of the course or instructor, and the date.
- Abstract : An abstract is typically not required in APSA style papers, but if one is included, it should be brief and summarize the main points of the paper.
- Introduction : The introduction should provide an overview of the research topic, the research question, and the main argument or thesis of the paper.
- Literature Review : The literature review should summarize the existing research on the topic and provide a context for the research question.
- Methods : The methods section should describe the research methods used in the paper, including data collection and analysis.
- Results : The results section should present the findings of the research.
- Discussion : The discussion section should interpret the results and connect them back to the research question and argument.
- Conclusion : The conclusion should summarize the main findings and implications of the research.
- References : The reference list should include all sources cited in the paper, formatted according to APSA style guidelines.
In-text citations in APSA style use parenthetical citation, which includes the author’s last name, publication year, and page number(s) if applicable. For example, (Smith 2010, 25).
About the author

Muhammad Hassan
Researcher, Academic Writer, Web developer
You may also like

How to Cite Research Paper – All Formats and...

Significance of the Study – Examples and Writing...

Research Paper Conclusion – Writing Guide and...

Research Paper – Structure, Examples and Writing...

Figures in Research Paper – Examples and Guide

Informed Consent in Research – Types, Templates...
How to format a research paper
Last updated
7 February 2023
Reviewed by
Miroslav Damyanov
Short on time? Get an AI generated summary of this article instead
Writing a research paper can be daunting if you’re not experienced with the process. Getting the proper format is one of the most challenging aspects of the task. Reviewers will immediately dismiss a paper that doesn't comply with standard formatting, regardless of the valuable content it contains.
In this article, we'll delve into the essential characteristics of a research paper, including the proper formatting.
Make research less tedious
Dovetail streamlines research to help you uncover and share actionable insights
- What is a research paper?
A research paper is a document that provides a thorough analysis of a topic , usually for an academic institution or professional organization. A research paper may be of any length, but they are typically 2,000–10,000 words.
Unlike less formal papers, such as articles or essays, empirical evidence and data are key to research papers. In addition to students handing in papers, scientists, attorneys, medical researchers, and independent scholars may need to produce research papers.
People typically write research papers to prove a particular point or make an argument. This could support or disprove a theoretical point, legal case, scientific theory, or an existing piece of research on any topic.
One of the distinguishing characteristics of research papers is that they contain citations to prior research. Citing sources using the correct format is essential for creating a legitimate research paper.
- Top considerations for writing a research paper
To write a research paper, you must consider several factors. Fields such as the sciences, humanities, and technical professions have certain criteria for writing research papers.
You’ll write a research paper using one of several types of formatting. These include APA, MLA, and CMOS styles, which we’ll cover in detail to guide you on citations and other formatting rules.
Specific requirements of the assignment
If the paper is for a college, university, or any specific organization, they’ll give you certain requirements, such as the range of topics, length, and formatting requirements.
You should study the specifics of the assignment carefully, as these will override more general guidelines you may find elsewhere. If you're writing for a particular professor, they may ask for single or double spacing or a certain citation style.
- Components of a research paper
Here are the basic steps to writing a quality research paper, assuming you've chosen your topic and considered the requirements of the paper. Depending on the specific conditions of the paper you're writing, you may need the following elements:
Thesis statement
The thesis statement provides a blueprint for the paper. It conveys the theme and purpose of the paper. It also informs you and readers what your paper will argue and the type of research it will contain. As you write the paper, you can refer to the thesis statement to help you decide whether or not to include certain items.
Most research papers require an abstract as well as a thesis. While the thesis is a short (usually a single sentence) summary of the work, an abstract contains more detail. Many papers use the IMRaD structure for the abstract, especially in scientific fields. This consists of four elements:
Introduction : Summarize the purpose of the paper
Methods : Describe the research methods (e.g., collecting data , interviews , field research)
Results: Summarize your conclusions.
Discussion: Discuss the implications of your research. Mention any significant limitations to your approach and suggest areas for further research.
The thesis and abstract come at the beginning of a paper, but you should write them after completing the paper. This approach ensures a clear idea of your main topic and argument, which can evolve as you write the paper.
Table of contents
Like most nonfiction books, a research paper usually includes a table of contents.
Tables, charts, and illustrations
If your paper contains multiple tables, charts, illustrations, or other graphics, you can create a list of these.
Works cited or reference page
This page lists all the works you cited in your paper. For MLA and APA styles, you will use in-text citations in the body of the paper. For Chicago (CMOS) style, you'll use footnotes.
Bibliography
While you use a reference page to note all cited papers, a bibliography lists all the works you consulted in your research, even if you don't specifically cite them.
While references are essential, a bibliography is optional but usually advisable to demonstrate the breadth of your research.
Dedication and acknowledgments
You may include a dedication or acknowledgments at the beginning of the paper directly after the title page and before the abstract.
- Steps for writing a research paper
These are the most critical steps for researching, writing, and formatting a research paper:
Create an outline
The outline is not part of the published paper; it’s for your use. An outline makes it easier to structure the paper, ensuring you include all necessary points and research.
Here you can list all topics and subtopics that will support your argument. When doing your research, you can refer to the outline to ensure you include everything.
Gather research
Solid research is the hallmark of a research paper. In addition to accumulating research, you need to present it clearly. However, gathering research is one of the first tasks. If you compile each piece of research correctly, it will be easier to format the paper correctly. You want to avoid having to go back and look up information constantly.
Start by skimming potentially useful sources and putting them aside for later use. Reading each source thoroughly at this stage will be time-consuming and slow your progress. You can thoroughly review the sources to decide what to include and discard later. At this stage, note essential information such as names, dates, page numbers, and website links. Citing sources will be easier when you’ve written all the information down.
Be aware of the quality of your sources. A research paper should reference scholarly, academic, or scientific journals. It’s vital to understand the difference between primary and secondary sources.
A primary source is an original, firsthand account of a topic. A secondary source is someone else covering the topic, as in a popular article or interview. While you may include secondary sources, your paper should also include primary research . Online research can be convenient, but you need to be extra careful when assessing the quality of your sources.
Write the first draft
Create a first draft where you put together all your research and address the topic described in your thesis and abstract.
Edit and format the paper
Proofread, edit, and make any necessary adjustments and improvements to the first draft. List your citations as described below. Ensure your thesis and abstract describe your research accurately.
- Formatting a research paper: MLA, APA, and CMOS styles
There are several popular formats for research papers: MLA (Modern Language Association) and APA (American Psychological Association). Certain academic papers use CMOS (Chicago Manual of Style). Other formats may apply to particular fields.
For example, medical research may use AMA (American Medical Association) formatting and IEEE (Institute of Electrical and Electronics Engineers) for particular technical papers. The following are the guidelines and examples of the most popular formats:
The humanities typically use MLA format, including literature, history, and culture. Look over examples of papers created in MLA format . Here are the main rules to keep in mind:
Double-spaced lines.
Indent new paragraphs 1/2 inch.
Title case for headings, where all major words are capitalized, as in "How to Write a Research Paper."
Use a popular font such as Times New Roman. This applies to all formatting styles.
Use one-inch margins on all sides.
Number sections of the paper using Arabic numerals (1, 2, 3, etc.).
Use a running head for each page on the upper right-hand corner, which consists of your last name and the page number.
Use an in-text citation within the text, using the author's last name followed by the page number: "Anything worth dying for is certainly worth living for" (Heller 155).
On the citations page, list the full name, book or periodical, and other information. For MLA, you will not need footnotes, only in-text citations.
List citations in alphabetical order on a separate page at the end of the paper entitled “Works Cited.”
Continuing with the above example from Heller, the listing would be: Heller, Joseph. Catch-22, Simon & Schuster, 1961.
For a periodical, the format is "Thompson, Hunter S. "The Kentucky Derby is Decadent and Depraved" Scanlon's, June 1970."
Use title case for source titles, as in "On the Origin of Species."
The sciences typically use APA format, including physical sciences such as physics and social sciences such as psychology. Simply Psychology provides examples of APA formatting . The following are the most important rules of the APA format.
Begin the paper with a title page, which is not required for MLA.
Use double-line spacing.
Use a running head for each page in the upper right-hand corner, which consists of the paper's title in capital letters followed by the page number.
The citations page at the end should be titled "References."
In-text citations should include the publication date: (Smith, 1999, p. 50). Note also that there's a "p" for "page," whereas in MLA, you write the page number without a "p."
As with MLA, use title case for headings, as in "Most Popular Treatments for Cognitive Disorders."
Use sentence case for titles of sources, as in "History of the decline and fall of the Roman empire." Note "Roman" starts with a capital because it's a proper noun.
When citing in-text references, use the author's last name and the first and middle initials.
Always use the Oxford comma. This comma goes before the words "or" and "and" in a list. For example, "At the store, I bought oranges, paper towels, and pasta."
CMOS formatting
Book publishers and many academic papers use CMOS formatting based on the Chicago Manual of Style. CMOS is also called Turabian, named after Kate L. Turabian, who wrote the first manual for this style. Here are examples of CMOS style formatting and citations.
Include an unnumbered title page.
Place page numbers on the upper right-hand corner of the page. Do not list your name or the paper's title as you would for MLA or APA styles.
Use title case for both headings and sources (same as MLA).
Unlike MLA and APA, the Chicago style uses footnotes for citations. Use a superscript for footnotes: "Smith argues against Jones' theory¹.” Footnotes may appear at the bottom of the page or the end of the document.
CMOS supports both short notes and full notes. In most cases, you'll use the full note: "Michael Pollan, The Omnivore's Dilemma: A Natural History of Four Meals (New York: Penguin, 2006), 76." For further references to the same source, use a short note: " Pollan, Omnivore's Dilemma, 45." The requirements of some papers may specify using only short notes for all footnotes.
- General guidelines for writing and formatting research papers
Keep these guidelines in mind for all types of research papers:
Initial formatting
As you create your first draft, don't worry about formatting. If you try to format it perfectly as you write the paper, it will be difficult to progress and develop a flow of thought. With the first draft, you don't have to be concerned about ordering the sections. You can rearrange headings and sections later.
Citation tools
Use automation tools for citations . Some useful tools make citations easier by automatically generating a citation list and bibliography. Many work with APA, MLA, and CMOS styles.
Check for plagiarism
Use a plagiarism detector to make sure your paper isn't unintentionally plagiarizing. There are many free and paid plagiarism checkers online, such as Grammarly.
Proofread your work
Do several rounds of editing and proofreading. Editing is necessary for any type of writing, but you’ll need to revisit several distinct areas with a research paper:
Check for spelling and grammatical errors.
Read the paper to make sure it's well-argued and that you’ve organized it properly.
Check that you’ve correctly formatted citations. It's easy to make errors, such as incorrect numbering of footnotes (e.g., Chicago style) or forgetting to include a source on your citations page.
Should you be using a customer insights hub?
Do you want to discover previous research faster?
Do you share your research findings with others?
Do you analyze research data?
Start for free today, add your research, and get to key insights faster
Editor’s picks
Last updated: 18 April 2023
Last updated: 27 February 2023
Last updated: 5 February 2023
Last updated: 16 April 2023
Last updated: 16 August 2024
Last updated: 9 March 2023
Last updated: 30 April 2024
Last updated: 12 December 2023
Last updated: 11 March 2024
Last updated: 4 July 2024
Last updated: 6 March 2024
Last updated: 5 March 2024
Last updated: 13 May 2024
Latest articles
Related topics, .css-je19u9{-webkit-align-items:flex-end;-webkit-box-align:flex-end;-ms-flex-align:flex-end;align-items:flex-end;display:-webkit-box;display:-webkit-flex;display:-ms-flexbox;display:flex;-webkit-flex-direction:row;-ms-flex-direction:row;flex-direction:row;-webkit-box-flex-wrap:wrap;-webkit-flex-wrap:wrap;-ms-flex-wrap:wrap;flex-wrap:wrap;-webkit-box-pack:center;-ms-flex-pack:center;-webkit-justify-content:center;justify-content:center;row-gap:0;text-align:center;max-width:671px;}@media (max-width: 1079px){.css-je19u9{max-width:400px;}.css-je19u9>span{white-space:pre;}}@media (max-width: 799px){.css-je19u9{max-width:400px;}.css-je19u9>span{white-space:pre;}} decide what to .css-1kiodld{max-height:56px;display:-webkit-box;display:-webkit-flex;display:-ms-flexbox;display:flex;-webkit-align-items:center;-webkit-box-align:center;-ms-flex-align:center;align-items:center;}@media (max-width: 1079px){.css-1kiodld{display:none;}} build next, decide what to build next, log in or sign up.
Get started for free
Have a language expert improve your writing
Run a free plagiarism check in 10 minutes, generate accurate citations for free.
- Knowledge Base
- Research paper
How to Write a Research Paper | A Beginner's Guide
A research paper is a piece of academic writing that provides analysis, interpretation, and argument based on in-depth independent research.
Research papers are similar to academic essays , but they are usually longer and more detailed assignments, designed to assess not only your writing skills but also your skills in scholarly research. Writing a research paper requires you to demonstrate a strong knowledge of your topic, engage with a variety of sources, and make an original contribution to the debate.
This step-by-step guide takes you through the entire writing process, from understanding your assignment to proofreading your final draft.
Instantly correct all language mistakes in your text
Upload your document to correct all your mistakes in minutes

Table of contents
Understand the assignment, choose a research paper topic, conduct preliminary research, develop a thesis statement, create a research paper outline, write a first draft of the research paper, write the introduction, write a compelling body of text, write the conclusion, the second draft, the revision process, research paper checklist, free lecture slides.
Completing a research paper successfully means accomplishing the specific tasks set out for you. Before you start, make sure you thoroughly understanding the assignment task sheet:
- Read it carefully, looking for anything confusing you might need to clarify with your professor.
- Identify the assignment goal, deadline, length specifications, formatting, and submission method.
- Make a bulleted list of the key points, then go back and cross completed items off as you’re writing.
Carefully consider your timeframe and word limit: be realistic, and plan enough time to research, write, and edit.
Receive feedback on language, structure, and formatting
Professional editors proofread and edit your paper by focusing on:
- Academic style
- Vague sentences
- Style consistency
See an example

There are many ways to generate an idea for a research paper, from brainstorming with pen and paper to talking it through with a fellow student or professor.
You can try free writing, which involves taking a broad topic and writing continuously for two or three minutes to identify absolutely anything relevant that could be interesting.
You can also gain inspiration from other research. The discussion or recommendations sections of research papers often include ideas for other specific topics that require further examination.
Once you have a broad subject area, narrow it down to choose a topic that interests you, m eets the criteria of your assignment, and i s possible to research. Aim for ideas that are both original and specific:
- A paper following the chronology of World War II would not be original or specific enough.
- A paper on the experience of Danish citizens living close to the German border during World War II would be specific and could be original enough.
Note any discussions that seem important to the topic, and try to find an issue that you can focus your paper around. Use a variety of sources , including journals, books, and reliable websites, to ensure you do not miss anything glaring.
Do not only verify the ideas you have in mind, but look for sources that contradict your point of view.
- Is there anything people seem to overlook in the sources you research?
- Are there any heated debates you can address?
- Do you have a unique take on your topic?
- Have there been some recent developments that build on the extant research?
In this stage, you might find it helpful to formulate some research questions to help guide you. To write research questions, try to finish the following sentence: “I want to know how/what/why…”
A thesis statement is a statement of your central argument — it establishes the purpose and position of your paper. If you started with a research question, the thesis statement should answer it. It should also show what evidence and reasoning you’ll use to support that answer.
The thesis statement should be concise, contentious, and coherent. That means it should briefly summarize your argument in a sentence or two, make a claim that requires further evidence or analysis, and make a coherent point that relates to every part of the paper.
You will probably revise and refine the thesis statement as you do more research, but it can serve as a guide throughout the writing process. Every paragraph should aim to support and develop this central claim.
Prevent plagiarism. Run a free check.
A research paper outline is essentially a list of the key topics, arguments, and evidence you want to include, divided into sections with headings so that you know roughly what the paper will look like before you start writing.
A structure outline can help make the writing process much more efficient, so it’s worth dedicating some time to create one.
Your first draft won’t be perfect — you can polish later on. Your priorities at this stage are as follows:
- Maintaining forward momentum — write now, perfect later.
- Paying attention to clear organization and logical ordering of paragraphs and sentences, which will help when you come to the second draft.
- Expressing your ideas as clearly as possible, so you know what you were trying to say when you come back to the text.
You do not need to start by writing the introduction. Begin where it feels most natural for you — some prefer to finish the most difficult sections first, while others choose to start with the easiest part. If you created an outline, use it as a map while you work.
Do not delete large sections of text. If you begin to dislike something you have written or find it doesn’t quite fit, move it to a different document, but don’t lose it completely — you never know if it might come in useful later.
Paragraph structure
Paragraphs are the basic building blocks of research papers. Each one should focus on a single claim or idea that helps to establish the overall argument or purpose of the paper.
Example paragraph
George Orwell’s 1946 essay “Politics and the English Language” has had an enduring impact on thought about the relationship between politics and language. This impact is particularly obvious in light of the various critical review articles that have recently referenced the essay. For example, consider Mark Falcoff’s 2009 article in The National Review Online, “The Perversion of Language; or, Orwell Revisited,” in which he analyzes several common words (“activist,” “civil-rights leader,” “diversity,” and more). Falcoff’s close analysis of the ambiguity built into political language intentionally mirrors Orwell’s own point-by-point analysis of the political language of his day. Even 63 years after its publication, Orwell’s essay is emulated by contemporary thinkers.
Citing sources
It’s also important to keep track of citations at this stage to avoid accidental plagiarism . Each time you use a source, make sure to take note of where the information came from.
You can use our free citation generators to automatically create citations and save your reference list as you go.
APA Citation Generator MLA Citation Generator
The research paper introduction should address three questions: What, why, and how? After finishing the introduction, the reader should know what the paper is about, why it is worth reading, and how you’ll build your arguments.
What? Be specific about the topic of the paper, introduce the background, and define key terms or concepts.
Why? This is the most important, but also the most difficult, part of the introduction. Try to provide brief answers to the following questions: What new material or insight are you offering? What important issues does your essay help define or answer?
How? To let the reader know what to expect from the rest of the paper, the introduction should include a “map” of what will be discussed, briefly presenting the key elements of the paper in chronological order.
The major struggle faced by most writers is how to organize the information presented in the paper, which is one reason an outline is so useful. However, remember that the outline is only a guide and, when writing, you can be flexible with the order in which the information and arguments are presented.
One way to stay on track is to use your thesis statement and topic sentences . Check:
- topic sentences against the thesis statement;
- topic sentences against each other, for similarities and logical ordering;
- and each sentence against the topic sentence of that paragraph.
Be aware of paragraphs that seem to cover the same things. If two paragraphs discuss something similar, they must approach that topic in different ways. Aim to create smooth transitions between sentences, paragraphs, and sections.
The research paper conclusion is designed to help your reader out of the paper’s argument, giving them a sense of finality.
Trace the course of the paper, emphasizing how it all comes together to prove your thesis statement. Give the paper a sense of finality by making sure the reader understands how you’ve settled the issues raised in the introduction.
You might also discuss the more general consequences of the argument, outline what the paper offers to future students of the topic, and suggest any questions the paper’s argument raises but cannot or does not try to answer.
You should not :
- Offer new arguments or essential information
- Take up any more space than necessary
- Begin with stock phrases that signal you are ending the paper (e.g. “In conclusion”)
There are four main considerations when it comes to the second draft.
- Check how your vision of the paper lines up with the first draft and, more importantly, that your paper still answers the assignment.
- Identify any assumptions that might require (more substantial) justification, keeping your reader’s perspective foremost in mind. Remove these points if you cannot substantiate them further.
- Be open to rearranging your ideas. Check whether any sections feel out of place and whether your ideas could be better organized.
- If you find that old ideas do not fit as well as you anticipated, you should cut them out or condense them. You might also find that new and well-suited ideas occurred to you during the writing of the first draft — now is the time to make them part of the paper.
The goal during the revision and proofreading process is to ensure you have completed all the necessary tasks and that the paper is as well-articulated as possible. You can speed up the proofreading process by using the AI proofreader .
Global concerns
- Confirm that your paper completes every task specified in your assignment sheet.
- Check for logical organization and flow of paragraphs.
- Check paragraphs against the introduction and thesis statement.
Fine-grained details
Check the content of each paragraph, making sure that:
- each sentence helps support the topic sentence.
- no unnecessary or irrelevant information is present.
- all technical terms your audience might not know are identified.
Next, think about sentence structure , grammatical errors, and formatting . Check that you have correctly used transition words and phrases to show the connections between your ideas. Look for typos, cut unnecessary words, and check for consistency in aspects such as heading formatting and spellings .
Finally, you need to make sure your paper is correctly formatted according to the rules of the citation style you are using. For example, you might need to include an MLA heading or create an APA title page .
Scribbr’s professional editors can help with the revision process with our award-winning proofreading services.
Discover our paper editing service
Checklist: Research paper
I have followed all instructions in the assignment sheet.
My introduction presents my topic in an engaging way and provides necessary background information.
My introduction presents a clear, focused research problem and/or thesis statement .
My paper is logically organized using paragraphs and (if relevant) section headings .
Each paragraph is clearly focused on one central idea, expressed in a clear topic sentence .
Each paragraph is relevant to my research problem or thesis statement.
I have used appropriate transitions to clarify the connections between sections, paragraphs, and sentences.
My conclusion provides a concise answer to the research question or emphasizes how the thesis has been supported.
My conclusion shows how my research has contributed to knowledge or understanding of my topic.
My conclusion does not present any new points or information essential to my argument.
I have provided an in-text citation every time I refer to ideas or information from a source.
I have included a reference list at the end of my paper, consistently formatted according to a specific citation style .
I have thoroughly revised my paper and addressed any feedback from my professor or supervisor.
I have followed all formatting guidelines (page numbers, headers, spacing, etc.).
You've written a great paper. Make sure it's perfect with the help of a Scribbr editor!
Open Google Slides Download PowerPoint
Is this article helpful?
Other students also liked.
- Writing a Research Paper Introduction | Step-by-Step Guide
- Writing a Research Paper Conclusion | Step-by-Step Guide
- Research Paper Format | APA, MLA, & Chicago Templates
More interesting articles
- Academic Paragraph Structure | Step-by-Step Guide & Examples
- Checklist: Writing a Great Research Paper
- How to Create a Structured Research Paper Outline | Example
- How to Write a Discussion Section | Tips & Examples
- How to Write Recommendations in Research | Examples & Tips
- How to Write Topic Sentences | 4 Steps, Examples & Purpose
- Research Paper Appendix | Example & Templates
- Research Paper Damage Control | Managing a Broken Argument
- What Is a Theoretical Framework? | Guide to Organizing
"I thought AI Proofreading was useless but.."
I've been using Scribbr for years now and I know it's a service that won't disappoint. It does a good job spotting mistakes”
- Search This Site All UCSD Sites Faculty/Staff Search Term
- Contact & Directions
- Climate Statement
- Cognitive Behavioral Neuroscience
- Cognitive Psychology
- Developmental Psychology
- Social Psychology
- Adjunct Faculty
- Non-Senate Instructors
- Researchers
- Psychology Grads
- Affiliated Grads
- New and Prospective Students
- Honors Program
- Experiential Learning
- Programs & Events
- Psi Chi / Psychology Club
- Prospective PhD Students
- Current PhD Students
- Area Brown Bags
- Colloquium Series
- Anderson Distinguished Lecture Series
- Speaker Videos
- Undergraduate Program
- Academic and Writing Resources
Writing Research Papers
- Research Paper Structure
Whether you are writing a B.S. Degree Research Paper or completing a research report for a Psychology course, it is highly likely that you will need to organize your research paper in accordance with American Psychological Association (APA) guidelines. Here we discuss the structure of research papers according to APA style.
Major Sections of a Research Paper in APA Style
A complete research paper in APA style that is reporting on experimental research will typically contain a Title page, Abstract, Introduction, Methods, Results, Discussion, and References sections. 1 Many will also contain Figures and Tables and some will have an Appendix or Appendices. These sections are detailed as follows (for a more in-depth guide, please refer to " How to Write a Research Paper in APA Style ”, a comprehensive guide developed by Prof. Emma Geller). 2
What is this paper called and who wrote it? – the first page of the paper; this includes the name of the paper, a “running head”, authors, and institutional affiliation of the authors. The institutional affiliation is usually listed in an Author Note that is placed towards the bottom of the title page. In some cases, the Author Note also contains an acknowledgment of any funding support and of any individuals that assisted with the research project.
One-paragraph summary of the entire study – typically no more than 250 words in length (and in many cases it is well shorter than that), the Abstract provides an overview of the study.
Introduction
What is the topic and why is it worth studying? – the first major section of text in the paper, the Introduction commonly describes the topic under investigation, summarizes or discusses relevant prior research (for related details, please see the Writing Literature Reviews section of this website), identifies unresolved issues that the current research will address, and provides an overview of the research that is to be described in greater detail in the sections to follow.
What did you do? – a section which details how the research was performed. It typically features a description of the participants/subjects that were involved, the study design, the materials that were used, and the study procedure. If there were multiple experiments, then each experiment may require a separate Methods section. A rule of thumb is that the Methods section should be sufficiently detailed for another researcher to duplicate your research.
What did you find? – a section which describes the data that was collected and the results of any statistical tests that were performed. It may also be prefaced by a description of the analysis procedure that was used. If there were multiple experiments, then each experiment may require a separate Results section.
What is the significance of your results? – the final major section of text in the paper. The Discussion commonly features a summary of the results that were obtained in the study, describes how those results address the topic under investigation and/or the issues that the research was designed to address, and may expand upon the implications of those findings. Limitations and directions for future research are also commonly addressed.
List of articles and any books cited – an alphabetized list of the sources that are cited in the paper (by last name of the first author of each source). Each reference should follow specific APA guidelines regarding author names, dates, article titles, journal titles, journal volume numbers, page numbers, book publishers, publisher locations, websites, and so on (for more information, please see the Citing References in APA Style page of this website).
Tables and Figures
Graphs and data (optional in some cases) – depending on the type of research being performed, there may be Tables and/or Figures (however, in some cases, there may be neither). In APA style, each Table and each Figure is placed on a separate page and all Tables and Figures are included after the References. Tables are included first, followed by Figures. However, for some journals and undergraduate research papers (such as the B.S. Research Paper or Honors Thesis), Tables and Figures may be embedded in the text (depending on the instructor’s or editor’s policies; for more details, see "Deviations from APA Style" below).
Supplementary information (optional) – in some cases, additional information that is not critical to understanding the research paper, such as a list of experiment stimuli, details of a secondary analysis, or programming code, is provided. This is often placed in an Appendix.
Variations of Research Papers in APA Style
Although the major sections described above are common to most research papers written in APA style, there are variations on that pattern. These variations include:
- Literature reviews – when a paper is reviewing prior published research and not presenting new empirical research itself (such as in a review article, and particularly a qualitative review), then the authors may forgo any Methods and Results sections. Instead, there is a different structure such as an Introduction section followed by sections for each of the different aspects of the body of research being reviewed, and then perhaps a Discussion section.
- Multi-experiment papers – when there are multiple experiments, it is common to follow the Introduction with an Experiment 1 section, itself containing Methods, Results, and Discussion subsections. Then there is an Experiment 2 section with a similar structure, an Experiment 3 section with a similar structure, and so on until all experiments are covered. Towards the end of the paper there is a General Discussion section followed by References. Additionally, in multi-experiment papers, it is common for the Results and Discussion subsections for individual experiments to be combined into single “Results and Discussion” sections.
Departures from APA Style
In some cases, official APA style might not be followed (however, be sure to check with your editor, instructor, or other sources before deviating from standards of the Publication Manual of the American Psychological Association). Such deviations may include:
- Placement of Tables and Figures – in some cases, to make reading through the paper easier, Tables and/or Figures are embedded in the text (for example, having a bar graph placed in the relevant Results section). The embedding of Tables and/or Figures in the text is one of the most common deviations from APA style (and is commonly allowed in B.S. Degree Research Papers and Honors Theses; however you should check with your instructor, supervisor, or editor first).
- Incomplete research – sometimes a B.S. Degree Research Paper in this department is written about research that is currently being planned or is in progress. In those circumstances, sometimes only an Introduction and Methods section, followed by References, is included (that is, in cases where the research itself has not formally begun). In other cases, preliminary results are presented and noted as such in the Results section (such as in cases where the study is underway but not complete), and the Discussion section includes caveats about the in-progress nature of the research. Again, you should check with your instructor, supervisor, or editor first.
- Class assignments – in some classes in this department, an assignment must be written in APA style but is not exactly a traditional research paper (for instance, a student asked to write about an article that they read, and to write that report in APA style). In that case, the structure of the paper might approximate the typical sections of a research paper in APA style, but not entirely. You should check with your instructor for further guidelines.
Workshops and Downloadable Resources
- For in-person discussion of the process of writing research papers, please consider attending this department’s “Writing Research Papers” workshop (for dates and times, please check the undergraduate workshops calendar).
Downloadable Resources
- How to Write APA Style Research Papers (a comprehensive guide) [ PDF ]
- Tips for Writing APA Style Research Papers (a brief summary) [ PDF ]
- Example APA Style Research Paper (for B.S. Degree – empirical research) [ PDF ]
- Example APA Style Research Paper (for B.S. Degree – literature review) [ PDF ]
Further Resources
How-To Videos
- Writing Research Paper Videos
APA Journal Article Reporting Guidelines
- Appelbaum, M., Cooper, H., Kline, R. B., Mayo-Wilson, E., Nezu, A. M., & Rao, S. M. (2018). Journal article reporting standards for quantitative research in psychology: The APA Publications and Communications Board task force report . American Psychologist , 73 (1), 3.
- Levitt, H. M., Bamberg, M., Creswell, J. W., Frost, D. M., Josselson, R., & Suárez-Orozco, C. (2018). Journal article reporting standards for qualitative primary, qualitative meta-analytic, and mixed methods research in psychology: The APA Publications and Communications Board task force report . American Psychologist , 73 (1), 26.
External Resources
- Formatting APA Style Papers in Microsoft Word
- How to Write an APA Style Research Paper from Hamilton University
- WikiHow Guide to Writing APA Research Papers
- Sample APA Formatted Paper with Comments
- Sample APA Formatted Paper
- Tips for Writing a Paper in APA Style
1 VandenBos, G. R. (Ed). (2010). Publication manual of the American Psychological Association (6th ed.) (pp. 41-60). Washington, DC: American Psychological Association.
2 geller, e. (2018). how to write an apa-style research report . [instructional materials]. , prepared by s. c. pan for ucsd psychology.
Back to top
- Formatting Research Papers
- Using Databases and Finding References
- What Types of References Are Appropriate?
- Evaluating References and Taking Notes
- Citing References
- Writing a Literature Review
- Writing Process and Revising
- Improving Scientific Writing
- Academic Integrity and Avoiding Plagiarism
- Writing Research Papers Videos
- Insights blog
How to write and structure a journal article
Sharing your research data can be hugely beneficial to your career , as well as to the scholarly community and wider society. But before you do so, there are some important ethical considerations to remember.
What are the rules and guidance you should follow, when you begin to think about how to write and structure a journal article? Ruth First Prize winner Steven Rogers, PhD said the first thing is to be passionate about what you write.
Steven Nabieu Rogers, Ruth First Prize winner.
Let’s go through some of the best advice that will help you pinpoint the features of a journal article, and how to structure it into a compelling research paper.
Planning for your article
When planning to write your article, make sure it has a central message that you want to get across. This could be a novel aspect of methodology that you have in your PhD study, a new theory, or an interesting modification you have made to theory or a novel set of findings.
2018 NARST Award winner Marissa Rollnick advised that you should decide what this central focus is, then create a paper outline bearing in mind the need to:
Isolate a manageable size
Create a coherent story/argument
Make the argument self-standing
Target the journal readership
Change the writing conventions from that used in your thesis

Get familiar with the journal you want to submit to
It is a good idea to choose your target journal before you start to write your paper. Then you can tailor your writing to the journal’s requirements and readership, to increase your chances of acceptance.
When selecting your journal think about audience, purposes, what to write about and why. Decide the kind of article to write. Is it a report, position paper, critique or review? What makes your argument or research interesting? How might the paper add value to the field?
If you need more guidance on how to choose a journal, here is our guide to narrow your focus.
Once you’ve chosen your target journal, take the time to read a selection of articles already published – particularly focus on those that are relevant to your own research.
This can help you get an understanding of what the editors may be looking for, then you can guide your writing efforts.
The Think. Check. Submit. initiative provides tools to help you evaluate whether the journal you’re planning to send your work to is trustworthy.
The journal’s aims and scope is also an important resource to refer back to as you write your paper – use it to make sure your article aligns with what the journal is trying to accomplish.
Keep your message focused
The next thing you need to consider when writing your article is your target audience. Are you writing for a more general audience or is your audience experts in the same field as you? The journal you have chosen will give you more information on the type of audience that will read your work.
When you know your audience, focus on your main message to keep the attention of your readers. A lack of focus is a common problem and can get in the way of effective communication.

Stick to the point. The strongest journal articles usually have one point to make. They make that point powerfully, back it up with evidence, and position it within the field.
How to format and structure a journal article
The format and structure of a journal article is just as important as the content itself, it helps to clearly guide the reader through.
How do I format a journal article?
Individual journals will have their own specific formatting requirements, which you can find in the instructions for authors.
You can save time on formatting by downloading a template from our library of templates to apply to your article text. These templates are accepted by many of our journals. Also, a large number of our journals now offer format-free submission, which allows you to submit your paper without formatting your manuscript to meet that journal’s specific requirements.
General structure for writing an academic journal article
The title of your article is one of the first indicators readers will get of your research and concepts. It should be concise, accurate, and informative. You should include your most relevant keywords in your title, but avoid including abbreviations and formulae.
Keywords are an essential part of producing a journal article. When writing a journal article you must select keywords that you would like your article to rank for.
Keywords help potential readers to discover your article when conducting research using search engines.
The purpose of your abstract is to express the key points of your research, clearly and concisely. An abstract must always be well considered, as it is the primary element of your work that readers will come across.
An abstract should be a short paragraph (around 300 words) that summarizes the findings of your journal article. Ordinarily an abstract will be comprised of:
What your research is about
What methods have been used
What your main findings are
Acknowledgements
Acknowledgements can appear to be a small aspect of your journal article, however it is still important. This is where you acknowledge the individuals who do not qualify for co-authorship, but contributed to your article intellectually, financially, or in some other manner.
When you acknowledge someone in your academic texts, it gives you more integrity as a writer as it shows that you are not claiming other academic’s ideas as your own intellectual property. It can also aid your readers in their own research journeys.

Introduction
An introduction is a pivotal part of the article writing process. An introduction not only introduces your topic and your stance on the topic, but it also (situates/contextualizes) your argument in the broader academic field.
The main body is where your main arguments and your evidence are located. Each paragraph will encapsulate a different notion and there will be clear linking between each paragraph.
Your conclusion should be an interpretation of your results, where you summarize all of the concepts that you introduced in the main body of the text in order of most to least important. No new concepts are to be introduced in this section.
References and citations
References and citations should be well balanced, current and relevant. Although every field is different, you should aim to cite references that are not more than 10 years old if possible. The studies you cite should be strongly related to your research question.
Clarity is key
Make your writing accessible by using clear language. Writing that is easy to read, is easier to understand too.
You may want to write for a global audience – to have your research reach the widest readership. Make sure you write in a way that will be understood by any reader regardless of their field or whether English is their first language.
Write your journal article with confidence, to give your reader certainty in your research. Make sure that you’ve described your methodology and approach; whilst it may seem obvious to you, it may not to your reader. And don’t forget to explain acronyms when they first appear.

Engage your audience. Go back to thinking about your audience; are they experts in your field who will easily follow technical language, or are they a lay audience who need the ideas presented in a simpler way?
Be aware of other literature in your field, and reference it
Make sure to tell your reader how your article relates to key work that’s already published. This doesn’t mean you have to review every piece of previous relevant literature, but show how you are building on previous work to avoid accidental plagiarism.
When you reference something, fully understand its relevance to your research so you can make it clear for your reader. Keep in mind that recent references highlight awareness of all the current developments in the literature that you are building on. This doesn’t mean you can’t include older references, just make sure it is clear why you’ve chosen to.
How old can my references be?
Your literature review should take into consideration the current state of the literature.
There is no specific timeline to consider. But note that your subject area may be a factor. Your colleagues may also be able to guide your decision.
Researcher’s view
Grasian Mkodzongi, Ruth First Prize Winner
Top tips to get you started
Communicate your unique point of view to stand out. You may be building on a concept already in existence, but you still need to have something new to say. Make sure you say it convincingly, and fully understand and reference what has gone before.
Editor’s view
Professor Len Barton, Founding Editor of Disability and Society
Be original
Now you know the features of a journal article and how to construct it. This video is an extra resource to use with this guide to help you know what to think about before you write your journal article.
Expert help for your manuscript
Taylor & Francis Editing Services offers a full range of pre-submission manuscript preparation services to help you improve the quality of your manuscript and submit with confidence.
Related resources
How to write your title and abstract
Journal manuscript layout guide
Improve the quality of English of your article
How to edit your paper
This document originally came from the Journal of Mammalogy courtesy of Dr. Ronald Barry, a former editor of the journal.
Purdue Online Writing Lab Purdue OWL® College of Liberal Arts
APA Formatting and Style Guide (7th Edition)

Welcome to the Purdue OWL
This page is brought to you by the OWL at Purdue University. When printing this page, you must include the entire legal notice.
Copyright ©1995-2018 by The Writing Lab & The OWL at Purdue and Purdue University. All rights reserved. This material may not be published, reproduced, broadcast, rewritten, or redistributed without permission. Use of this site constitutes acceptance of our terms and conditions of fair use.
In-Text Citations
Resources on using in-text citations in APA style
Reference List
Resources on writing an APA style reference list, including citation formats
Other APA Resources

Scholarly Journal Articles: Structure and Function
- Scholarly Publications
- Forms of Literature
- Peer-review
- Structure of a research article
- Sample Articles
- Title and Abstract
- Authors and Funding
- Introduction and Methods
- Results and Discussion
Structure of a research article in the health sciences
Research in the health sciences can be qualitative, quantitative, or a combination of the two. This guide will focus primarily on quantitative research.
Quantitative research articles are usually written in a standardized format called the IMRaD format. This acronym refers to the I ntroduction, M ethods, R esults, (and) D iscussion sections of the articles. There is also usually a Conclusions section. By following this conventional structure, authors ensure that readers of their articles will be able to readily locate the paper's critical elements.
This rule is not hard and fast, and sometimes the sections may be rearranged or combined, or the authors may use alternate wording for the headings. Regardless, the basic elements are usually present.
Some types of original studies , such as case reports, do not readily lend themselves to this format. But even these types of papers will often follow a logical progression, in which they begin by stating the problem, then move on to describing their findings, and finally to offering possible explanations or conclusions.
Journal articles that are not primary literature, most notably review articles, will be written in whatever style is most appropriate to the content.
- << Previous: Peer-review
- Next: Sample Articles >>
- Last Updated: Jan 11, 2024 11:08 AM
- URL: https://researchguides.uvm.edu/ScholarlyJournalArticle

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- J Med Libr Assoc
- v.103(2); 2015 Apr
How to write an original research paper (and get it published)
The purpose of the Journal of the Medical Library Association (JMLA) is more than just archiving data from librarian research. Our goal is to present research findings to end users in the most useful way. The “Knowledge Transfer” model, in its simplest form, has three components: creating the knowledge (doing the research), translating and transferring it to the user, and incorporating the knowledge into use. The JMLA is in the middle part, transferring and translating to the user. We, the JMLA, must obtain the information and knowledge from researchers and then work with them to present it in the most useable form. That means the information must be in a standard acceptable format and be easily readable.
There is a standard, preferred way to write an original research paper. For format, we follow the IMRAD structure. The acronym, IMRAD, stands for I ntroduction, M ethods, R esults A nd D iscussion. IMRAD has dominated academic, scientific, and public health journals since the second half of the twentieth century. It is recommended in the “Uniform Requirements for Manuscripts Submitted to Biomedical Journals” [ 1 ]. The IMRAD structure helps to eliminate unnecessary detail and allows relevant information to be presented clearly in a logical sequence [ 2 , 3 ].
Here are descriptions of the IMRAD sections, along with our comments and suggestions. If you use this guide for submission to another journal, be sure to check the publisher's prescribed formats.
The Introduction sets the stage for your presentation. It has three parts: what is known, what is unknown, and what your burning question, hypothesis, or aim is. Keep this section short, and write for a general audience (clear, concise, and as nontechnical as you can be). How would you explain to a distant colleague why and how you did the study? Take your readers through the three steps ending with your specific question. Emphasize how your study fills in the gaps (the unknown), and explicitly state your research question. Do not answer the research question. Remember to leave details, descriptions, speculations, and criticisms of other studies for the Discussion .
The Methods section gives a clear overview of what you did. Give enough information that your readers can evaluate the persuasiveness of your study. Describe the steps you took, as in a recipe, but be wary of too much detail. If you are doing qualitative research, explain how you picked your subjects to be representative.
You may want to break it into smaller sections with subheadings, for example, context: when, where, authority or approval, sample selection, data collection (how), follow-up, method of analysis. Cite a reference for commonly used methods or previously used methods rather than explaining all the details. Flow diagrams and tables can simplify explanations of methods.
You may use first person voice when describing your methods.
The Results section summarizes what the data show. Point out relationships, and describe trends. Avoid simply repeating the numbers that are already available in the tables and figures. Data should be restricted to tables as much as possible. Be the friendly narrator, and summarize the tables; do not write the data again in the text. For example, if you had a demographic table with a row of ages, and age was not significantly different among groups, your text could say, “The median age of all subjects was 47 years. There was no significant difference between groups (Table).” This is preferable to, “The mean age of group 1 was 48.6 (7.5) years and group 2 was 46.3 (5.8) years, a nonsignificant difference.”
Break the Results section into subsections, with headings if needed. Complement the information that is already in the tables and figures. And remember to repeat and highlight in the text only the most important numbers. Use the active voice in the Results section, and make it lively. Information about what you did belongs in the Methods section, not here. And reserve comments on the meaning of your results for the Discussion section.
Other tips to help you with the Results section:
- ▪ If you need to cite the number in the text (not just in the table), and the total in the group is less than 50, do not include percentage. Write “7 of 34,” not “7 (21%).”
- ▪ Do not forget, if you have multiple comparisons, you probably need adjustment. Ask your statistician if you are not sure.
The Discussion section gives you the most freedom. Most authors begin with a brief reiteration of what they did. Every author should restate the key findings and answer the question noted in the Introduction . Focus on what your data prove, not what you hoped they would prove. Start with “We found that…” (or something similar), and explain what the data mean. Anticipate your readers' questions, and explain why your results are of interest.
Then compare your results with other people's results. This is where that literature review you did comes in handy. Discuss how your findings support or challenge other studies.
You do not need every article from your literature review listed in your paper or reference list, unless you are writing a narrative review or systematic review. Your manuscript is not intended to be an exhaustive review of the topic. Do not provide a long review of the literature—discuss only previous work that is directly pertinent to your findings. Contrary to some beliefs, having a long list in the References section does not mean the paper is more scholarly; it does suggest the author is trying to look scholarly. (If your article is a systematic review, the citation list might be long.)
Do not overreach your results. Finding a perceived knowledge need, for example, does not necessarily mean that library colleges must immediately overhaul their curricula and that it will improve health care and save lives and money (unless your data show that, in which case give us a chance to publish it!). You can say “has the potential to,” though.
Always note limitations that matter, not generic limitations.
Point out unanswered questions and future directions. Give the big-picture implications of your findings, and tell your readers why they should care. End with the main findings of your study, and do not travel too far from your data. Remember to give a final take-home message along with implications.
Notice that this format does not include a separate Conclusion section. The conclusion is built into the Discussion . For example, here is the last paragraph of the Discussion section in a recent NEJM article:
In conclusion, our trial did not show the hypothesized benefit [of the intervention] in patients…who were at high risk for complications.
However, a separate Conclusion section is usually appropriate for abstracts. Systematic reviews should have an Interpretation section.
Other parts of your research paper independent of IMRAD include:
Tables and figures are the foundation for your story. They are the story. Editors, reviewers, and readers usually look at titles, abstracts, and tables and figures first. Figures and tables should stand alone and tell a complete story. Your readers should not need to refer back to the main text.
Abstracts can be free-form or structured with subheadings. Always follow the format indicated by the publisher; the JMLA uses structured abstracts for research articles. The main parts of an abstract may include introduction (background, question or hypothesis), methods, results, conclusions, and implications. So begin your abstract with the background of your study, followed by the question asked. Next, give a quick summary of the methods used in your study. Key results come next with limited raw data if any, followed by the conclusion, which answers the questions asked (the take-home message).
- ▪ Recommended order for writing a manuscript is first to start with your tables and figures. They tell your story. You can write your sections in any order. Many recommend writing your Result s, followed by Methods, Introduction, Discussion , and Abstract.
- ▪ We suggest authors read their manuscripts out loud to a group of librarians. Look for evidence of MEGO, “My Eyes Glaze Over” (attributed to Washington Post publisher Ben Bradlee and others). Modify as necessary.
- ▪ Every single paragraph should be lucid.
- ▪ Every paragraph should answer your readers' question, “Why are you telling me this?”
The JMLA welcomes all sizes of research manuscripts: definitive studies, preliminary studies, critical descriptive studies, and test-of-concept studies. We welcome brief reports and research letters. But the JMLA is more than a research journal. We also welcome case studies, commentaries, letters to the editor about articles, and subject reviews.
- SpringerLink shop
Types of journal articles
It is helpful to familiarise yourself with the different types of articles published by journals. Although it may appear there are a large number of types of articles published due to the wide variety of names they are published under, most articles published are one of the following types; Original Research, Review Articles, Short reports or Letters, Case Studies, Methodologies.
Original Research:
This is the most common type of journal manuscript used to publish full reports of data from research. It may be called an Original Article, Research Article, Research, or just Article, depending on the journal. The Original Research format is suitable for many different fields and different types of studies. It includes full Introduction, Methods, Results, and Discussion sections.
Short reports or Letters:
These papers communicate brief reports of data from original research that editors believe will be interesting to many researchers, and that will likely stimulate further research in the field. As they are relatively short the format is useful for scientists with results that are time sensitive (for example, those in highly competitive or quickly-changing disciplines). This format often has strict length limits, so some experimental details may not be published until the authors write a full Original Research manuscript. These papers are also sometimes called Brief communications .
Review Articles:
Review Articles provide a comprehensive summary of research on a certain topic, and a perspective on the state of the field and where it is heading. They are often written by leaders in a particular discipline after invitation from the editors of a journal. Reviews are often widely read (for example, by researchers looking for a full introduction to a field) and highly cited. Reviews commonly cite approximately 100 primary research articles.
TIP: If you would like to write a Review but have not been invited by a journal, be sure to check the journal website as some journals to not consider unsolicited Reviews. If the website does not mention whether Reviews are commissioned it is wise to send a pre-submission enquiry letter to the journal editor to propose your Review manuscript before you spend time writing it.
Case Studies:
These articles report specific instances of interesting phenomena. A goal of Case Studies is to make other researchers aware of the possibility that a specific phenomenon might occur. This type of study is often used in medicine to report the occurrence of previously unknown or emerging pathologies.
Methodologies or Methods
These articles present a new experimental method, test or procedure. The method described may either be completely new, or may offer a better version of an existing method. The article should describe a demonstrable advance on what is currently available.
Back │ Next

IMRAD Format For Research Papers: The Complete Guide

Thank you for reading DrAiMD’s Substack. This post is public so feel free to share it.
Writing a strong research paper is key to succeeding in academia, but it can be overwhelming to know where to start. That’s where the IMRAD format comes in. IMRAD provides a clear structure to help you organize and present your research logically and coherently. In this comprehensive guide, we’ll explain the IMRAD format, why it’s so important for research writing, and how to use it effectively. Follow along to learn the ins and outs of crafting papers in the gold-standard IMRAD structure. In this article, I’ll walk you through the IMRAD format step-by-step. I’ll explain each section, how to write it, and what to avoid. By the end of this article, you’ll be able to write a research paper that is clear, concise, and well-organized.
What is IMRAD Format?
IMRAD stands for Introduction, Methods, Results, and Discussion . It’s a way of organizing a scientific paper to make the information flow logically and help readers easily find key details. The IMRAD structure originated in medical journals but is now the standard format for many scientific fields.
Thanks for reading DrAiMD’s Substack! Subscribe for free to receive new posts and support my work.
Here’s a quick overview of each section’s purpose:
Introduction : Summary of prior research and objective of your study
Methods : How you carried out the study
Results : Key findings and analysis
Discussion : Interpretation of results and implications
Most papers also include an abstract at the beginning and a conclusion at the end to summarize the entire report.
Why is the IMRAD Format Important?
Using the IMRAD structure has several key advantages:
It’s conventional and familiar. Since I MRAD is so widely used , it helps ensure editors, reviewers, and readers can easily find the details they need. This enhances clarity and comprehension.
It emphasizes scientific rigor. The methods and results sections encourage thorough reporting of how you conducted the research. This supports transparency, credibility, and reproducibility.
It encourages precision. The structure necessitates concise writing focused only on the core aims and findings. This avoids rambling or repetition.
It enables efficient reading. Readers can quickly skim to the sections most relevant to them, like only reading the methods. IMRAD facilitates this selective reading.
In short, the IMRAD format ensures your writing is clear, precise, rigorous, and accessible – crucial qualities in scientific communication.
When Should You Use IMRAD Format?
The IMRAD structure is ideal for:
Primary research papers that report new data and findings
Review papers that comprehensively summarize prior research
Grant proposals requesting funding for research
IMRAD is not typically used for other paper types like:
Editorials and opinion pieces
Popular science articles for general audiences
Essays analyzing a topic rather than presenting new data
So, if you are writing a scholarly scientific paper based on experiments, investigations, or observational studies, the IMRAD format is likely expected. Embrace this conventional structure to help communicate your exciting discoveries.
Now that we’ve covered the key basics let’s dive into how to write each section of an IMRAD paper.
The abstract is a succinct summary of your entire paper, typically around 200 words. Many readers will only read the abstract, so craft it carefully to function as a standalone piece highlighting your most important points.
Elements to include:
Research problem, question, or objectives
Methods and design
Major findings or developments
Conclusions and implications
While written first, refine the abstract last to accurately encapsulate your final paper. A clear precise abstract can help attract readers and set the tone for your work. Take a look at our complete guide to abstract writing here !
INTRODUCTION
The Introduction provides the necessary background context and sets up the rationale for your research. Start by briefly summarizing the core findings from previous studies related to your topic to orient readers to the field. Provide more detail on the specific gaps, inconsistencies, or unanswered questions in the research your study aims to address. Then, clearly state your research questions, objectives, experimental hypotheses, and overall purpose or anticipated contributions. The Introduction establishes why your research is needed and clarifies your specific aims. Strive for a concise yet comprehensive overview that lets readers learn more about your fascinating study. Writing a good introduction is like writing a good mini-literature review on a subject. Take a look at our complete guide to literature review writing here!

The methods section is the nuts and bolts, where you comprehensively describe how you carried out the research. Sufficient detail is crucial so others can assess your work and reproduce the study. Take a look at our complete guide to writing an informative and tight literature review here!
Research Design
Start by explaining the overall design and approach. Specify:
Research types like experimental, survey, observational, etc.
Study duration
Sample size
Control vs experimental groups
Clarify the variables, treatments, and factors involved.
Participants
Provide relevant characteristics of the study population or sample, such as:
Health status
Geographic location
For human studies, include recruitment strategies and consent procedures.
List any instruments, tests, assays, chemicals, or other materials utilized. Include details like manufacturers and catalog numbers.
Chronologically explain each step of the experimental methods. Be precise and thorough to enable replication. Use past tense and passive voice.
Data Analysis
Describe any statistical tests, data processing, or software used to analyze the data.
The methods section provides the roadmap of your research journey. Strive for clarity and completeness. Now we’re ready for the fun part – the results!
This section shares the key findings and data from your study without interpretation. The results should mirror the methods used.
Report Findings Concisely
Use text, figures, and tables to present the core results:
Focus only on key data directly related to your objectives
Avoid lengthy explanations and extraneous details
Highlight the most groundbreaking findings
Use Visuals to Present Complex Data

Tables and figures efficiently communicate more complex data:
Tables organize detailed numerical or textual data
Figures vividly depict relationships like graphs, diagrams, photos
Include clear captions explaining what is shown
Refer to each visual in the text
Reporting your results objectively lays the groundwork for the next section – making sense of it all through discussion.
Here, you interpret the data, explain the implications, acknowledge limitations, and make recommendations for future research. The discussion allows you to show the greater meaning of your study.
Interpret the Findings
Analyze the results in the context of your initial hypothesis and prior studies:
How do your findings compare to past research? Are they consistent or contradictory?
What conclusions can you draw from the data?
What theories or mechanisms could explain the outcomes?
Discuss the Implications
Address the impact and applications of the research:
How do the findings advance scientific understanding or technical capability?
Can the results improve processes, design, or policies in related fields?
What innovations or new research directions do they enable?
Identify Limitations and Future Directions
No study is perfect, so discuss potential weaknesses and areas for improvement:
Were there any methodological limitations that could influence the results?
Can the research be expanded by testing new variables or conditions?
How could future studies build on your work? What questions remain unanswered?
A thoughtful discussion emphasizes the meaningful contributions of your research.
The conclusion recaps the significance of your study and key takeaways. Like the abstract, many readers may only read your opening and closing, so ensure the conclusion packs a punch.
Elements to cover:
Restate the research problem and objectives
Summarize the major findings and main points
Emphasize broader implications and applications
The conclusion provides the perfect opportunity to drive home the importance of your work. End on a high note that resonates with readers.
The IMRAD format organizes research papers into logical sections that improve scientific communication. By following the Introduction-Methods-Results-and-Discussion structure, you can craft clear, credible, and impactful manuscripts. Use IMRAD to empower readers to comprehend and assess your exciting discoveries efficiently. With this gold-standard format under your belt, your next great paper is within reach.
Ready for more?
Quantitative Research Article Review: Guidelines & Tips
Effects of a mobile-app-based self-compassion intervention on psychological health and maladaptive cognitive traits: findings from a randomized controlled trial
- Open access
- Published: 20 August 2024
Cite this article
You have full access to this open access article

- Wei Tian Han ORCID: orcid.org/0009-0007-1982-4834 1 ,
- Shian-Ling Keng ORCID: orcid.org/0000-0002-7564-2425 2 , 3 ,
- Karen Pooh ORCID: orcid.org/0009-0002-3775-3332 1 ,
- Ziying Wang ORCID: orcid.org/0009-0000-8929-9667 1 &
- Madhumitha Ayyappan 1
College students are at risk of poor mental health and other maladaptive traits such as academic worry, perfectionism, and rumination. This study aimed to examine the effects of a seven-week mobile app-based self-compassion intervention on psychological symptoms and maladaptive cognitive traits in a sample of college students based in Singapore. Using a randomized controlled trial design, a total of 63 participants (mean age = 21.2; 64.2% female) were recruited and randomly assigned to either the self-compassion program ( n = 31) or a waitlist control condition ( n = 32). The online self-compassion program was administered via the mobile app 29k , which consists of weekly lessons each lasting 30 to 60 min. Outcome measures were administered a week before and after the intervention program. Analyses indicated that compared to participants in the waitlist control condition, participants in the intervention condition reported significantly greater decreases in depressive symptoms, anxiety, and stress. There was also a trend for greater decreases in academic worry in the intervention condition. No significant between-group differences were found on changes in trait self-compassion, perfectionism, or rumination. The results are promising in indicating that app-based self-compassion programs may be effective in improving selected aspects of college students’ mental health. Future research could investigate additional features that could be incorporated into mobile app-based interventions, such as synchronous sessions with a trained facilitator, and more targeted content for college students.
Avoid common mistakes on your manuscript.
College is a challenging time for many students, with many stressors arising from factors such as relationships, high expectations, and academics, among others (Hurst et al., 2013 ). It is thus unsurprising that many college students struggle with mental health-related problems. A recent systematic review involving cross-national studies found that 25% of college students experienced depression and 14% of college students experienced suicidal thoughts or behaviors (Sheldon et al., 2021 ). This has only worsened with the COVID-19 pandemic, as noted by one meta-analysis revealing increased rates of depression and anxiety among college students after the start of the pandemic (Li et al., 2021 ).
The COVID-19 pandemic has negatively impacted college students’ mental health. College students have reported greater stress associated with the shift to online learning, citing reasons such as loneliness, difficulty coping, uncertainty towards examinations and classes, and worries about their academic future being at risk due to COVID-19 related factors (Birmingham et al., 2021 ; Clabaugh et al., 2021 ; Moawad, 2020 ). Furthermore, students have reported greater dissatisfaction with online learning as opposed to face-to-face learning, due to being unable to focus during online classes, poorer quality of class discussions, and difficulties in clarifying and understanding class material (Nambiar, 2020 ). Thus, college students are a vulnerable population at high risk of psychological problems.
To date, a number of interventions have been developed to improve college students’ mental health (Huang et al., 2018 ). Of these interventions, one promising approach is self-compassion-based interventions, which have been shown to improve psychological outcomes across a wide range of populations (Ferrari et al., 2019 ). The concept of self-compassion was first articulated by Dr Kristin Neff ( 2003a ) as an alternative to self-esteem in conceptualizing psychological well-being. Self-compassion involves treating ourselves with kindness, understanding, and care in times of difficulty or suffering (Neff, 2003a ). As proposed by Neff, self-compassion encompasses three main components, namely mindfulness, common humanity, and self-kindness. Mindfulness entails non-judgmental acceptance of one’s moment-to-moment experience. Common humanity fosters connection through recognizing the universal nature of human struggles. Embracing self-kindness helps individuals respond to their own suffering with empathy and support, promoting emotional well-being and resilience. Much research has shown that trait self-compassion is positively correlated with psychological well-being, cognitive well-being, and positive affective well-being, and negatively correlated with negative affect and psychopathological symptoms in both clinical and non-clinical populations (MacBeth & Gumley, 2012 ; Zessin et al., 2015 ).
Self-compassion interventions focus on teaching specific self-compassion practice techniques that can be incorporated into daily life. These interventions are typically delivered via group sessions with trained facilitators and include guided practices and exercises. The duration of these interventions varies from intensive three-day courses to eight-week programs. The effects of such self-compassion interventions on psychological health have also been well-studied. A meta-analysis of randomized controlled trials of different self-compassion interventions found that self-compassion interventions led to significant improvements in several psychological outcomes, with moderate effect sizes for depression, anxiety, and stress (Ferrari et al., 2019 ).
The present study used an adaptation of the Mindful Self-Compassion (MSC) program as a self-compassion intervention. The MSC program was originally developed by Neff and Germer ( 2013 ), and incorporates a blend of exercises, discussions, and homework assignments to teach and equip participants with a variety of self-compassionate tools. In a pilot study, a randomized controlled trial found that the MSC intervention led to significant improvements in trait self-compassion, trait mindfulness, life satisfaction, as well as depression, anxiety, and stress (Neff & Germer, 2013 ). These results were corroborated in a subsequent study by Smeets et al. ( 2014 ), in which a three-week self-compassion intervention program adapted from the MSC program led to increases in female college students’ trait mindfulness, optimism, and self-efficacy, as well as decreases in rumination, as compared to an active control group that underwent a program on general time management. Another study involving a Chinese college student sample found that compared to a waitlist control group, a group-based self-compassion intervention program led to reduced depression and stress, and enhanced future-oriented coping (Huang et al., 2021 ). Taken together, these studies indicate the promise of self-compassion-based interventions in improving psychological health in college students.
Online self-compassion interventions
With the COVID-19 pandemic, the use of virtual platforms as a substitution for in-person activities has become much more widespread. Many face-to-face self-compassion interventions have been adapted to an online format to be accessible during a global pandemic, when social distancing was a norm. Digital mindfulness-based interventions have many advantages (Begin et al., 2022 ). They provide a lower barrier to entry to those seeking psychological support, as digital interventions are free or low-cost, easily and rapidly implemented in different settings, and eliminate issues of space availability, travel and schedule coordination that are linked with participating in traditional face-to-face mindfulness programs. Digital interventions also offer more privacy and flexibility as they can be self-paced and be done anywhere at any time, which makes them more attractive to busier individuals such as college students. More importantly, digital programs may be able to target a niche population of individuals with severe psychological problems, who may avoid seeking in-person treatment, perhaps due to severe anxiety or fear of the stigma associated with mental illness (Krieger et al., 2016 ; Rauschenberg et al., 2021 ).
While web-based programs may be effective, there are additional benefits that could come specifically from phone-based apps, such as the convenience in being able to access the lessons when individuals are on the go. One specific mobile app of interest, 29k , also offers an adaptation of the MSC program (Neff & Germer, 2013 ) which teaches both formal meditation practices as well as other informal practices which can be used in daily life. The course content is delivered via weekly lessons on the app, which consists of psychoeducational videos with a facilitator, guided audio meditation exercises, as well as writing and reflection exercises. Such accessible digital interventions are especially crucial now due to the increasing demand for mental health services in response to declining mental health in the general population, exacerbated by a shortage of mental health professionals (Keshavan, 2020 ; Rodriguez-Villa et al., 2020 ; Wang et al., 2021 ).
To date, there has been preliminary research examining the effects of online self-compassion-based interventions for college students. A pilot randomized controlled trial involving Swedish college students found that an app-based self-compassion intervention resulted in greater improvements in trait self-compassion and stress compared to a waitlist control group (Andersson et al., 2021 ). Another single-arm open trial of a six-week web-based self-compassion program conducted in a sample of postgraduate psychology trainees found that there were significant improvements in trait self-compassion, happiness, perceived stress, and depression from pre- to post-intervention, and that these changes were maintained at follow-up assessment three months later (Finlay-Jones et al., 2017 ). However, this study did not include a control group, which precludes causal conclusions regarding the effects of the program in improving psychological health.
Beyond self-compassion-based interventions, past studies have also examined the effects of interventions developed based on components of self-compassion (e.g., mindfulness) on psychological health outcomes. A randomized controlled trial showed that a mindfulness app-based intervention was effective in reducing depression, anxiety and stress compared to a waitlist control group in a sample of Canadian adults (Al-Refae et al., 2021 ). Additionally, a meta-analysis of randomized controlled trials examining the efficacy of phone-based mindfulness and acceptance applications found that there were significantly greater increases in trait self-compassion when interventions were delivered via a mobile app than in comparison groups (Linardon, 2020 ). These findings suggest that trait self-compassion may be improved via online interventions, even if the intervention programs implemented were not explicitly targeted at cultivating self-compassion. Notably, Linardon ( 2020 ) acknowledged that effect sizes were small, and that more studies on smartphone apps focusing specifically on self-compassion are necessary to draw further conclusions regarding the effects of online interventions on self-compassion. Further, relatively less research has examined whether self-compassion-based interventions may modify maladaptive cognitive processes, which are known to underlie the development of many psychopathological symptoms (Egan et al., 2011 ; Limburg et al., 2017 ; Luca, 2019 ).
Academic worry, perfectionism, and rumination
College students, besides being more prone to experiencing poor psychological health symptoms of depression, anxiety, and stress, often exhibit maladaptive traits such as excessive academic worry. Academic worry encompasses concerns about exams, performance, workload, and related matters (Bedewy & Gabriel, 2015 ). In Singapore, academic achievements are highly prioritized, and students face overwhelming academic pressure from a young age (Poh, 2018 ), with research demonstrating higher academic stress experienced by Singaporean adolescents compared with adolescents from other cultures (e.g., Canada; Ang et al., 2009 ). The intense emphasis on academic achievement in the Singaporean culture exacerbates this worry, impacting college students’ psychological well-being. Research has demonstrated a positive correlation between academic worry and elevated levels of depression, anxiety, and stress in college students (Beiter et al., 2015 ). Hence, addressing excessive academic worry is vital for supporting college students’ mental health.
Additionally, perfectionism and rumination are other important traits that need to be examined, as they are transdiagnostic risk factors that have been shown to predict worsened mental well-being among college students (Egan et al., 2011 ; Limburg et al., 2017 ; McLaughlin & Nolen-Hoeksema, 2011 ). Slaney et al. ( 2001 ) define perfectionism as (1) having exceedingly high expectations of one’s performance or behavior, and (2) experiencing difficulties completing tasks due to the high expectations. Past research has found a significant association between maladaptive perfectionism and academic-related anxiety in college students (Dobos et al., 2021 ; Eum & Rice, 2011 ). A meta-analysis also shows that perfectionism is associated with several psychological disorders (e.g., depression and anxiety disorders), poor psychological symptoms, and suicidal ideation (Limburg et al., 2017 ). Of equal concern is rumination, defined as the process of focusing on one’s own negative mood in a repetitive manner, which often involves excessive and pessimistic contemplative thoughts (Treynor et al., 2003 ). In previous research, rumination has been well-established as a predictor of depressive symptoms (Nolen-Hoeksema, 2000 ). Rumination has also been found to predict anxiety and stress in college students (McLaughlin & Nolen-Hoeksema, 2011 ; Samaie & Farahani, 2011 ).
Self-compassion interventions are potentially helpful in addressing maladaptive cognitive processes, as the practice of mindfully being kind to oneself may help alleviate negative self-judgement directed towards one’s grades and achievements, as well as combat negative ruminative thoughts and perfectionistic self-criticism. Past studies have found that trait self-compassion is negatively correlated with academic stress (Lee & Lee, 2022 ), academic motivation anxiety (Williams et al., 2008 ), and perfectionism (Richardson et al., 2020 ; Stoeber et al., 2020 ). Correspondingly, a meta-analysis also found that randomized controlled trials of self-compassion interventions led to significant decreases in rumination, with large effect sizes identified (Ferrari et al., 2019 ). However, there is a lack of studies examining whether self-compassion interventions can remain effective in addressing maladaptive cognitive processes when administered in smaller dosages, such as via a program on a phone app. Assessing the efficacy of phone-based interventions has important implications as these interventions could provide a more accessible solution for reducing these maladaptive traits among college students.
Aims and hypotheses
This study aimed to examine the effects of a seven-week, mobile app-based self-compassion intervention on psychological symptoms and maladaptive cognitive processes in a sample of Singapore-based college students, using a randomized controlled design. It was hypothesized that students participating in the self-compassion intervention would report significantly greater decreases in depressive symptoms, anxiety, and stress, as well as increases in trait self-compassion compared to a waitlist control group. It was also predicted that participants of the self-compassion intervention would report significantly greater reductions on academic worry, perfectionism, and rumination compared to the control group.
Participants
A total of 63 participants were recruited via fliers and social media advertisements posted within two Singapore universities. The study’s eligibility criteria were aged 18 years and above and a current undergraduate or postgraduate student. Participants who had previously completed an eight-week MSC program were not eligible for the study. Interested participants were directed to a Google form to answer several pre-screening questions to assess their eligibility. The study was reviewed and approved by the institution’s Undergraduate Research Ethics Committee.
The sample size for the study was derived based on power calculation conducted using G*Power (Faul et al., 2007 ). Assuming a small-to-medium effect size, 80% power and an alpha level of 0.05, the calculation indicated that a sample size of 60 would be required to detect a significant Group by Time interaction, using a mixed ANOVA analytic approach. The effect size estimate was derived from a study assessing the effects of an online six-week self-compassion training on trait self-compassion, perceived stress, depression, and anxiety (Finlay-Jones et al., 2017 ).
Figure 1 illustrates the study’s procedure in the form of a CONSORT diagram. Upon recruitment, participants eligible for the study were randomly assigned to either the intervention group ( n = 31) or a waitlist control group ( n = 32) using an online randomizer. Participants were invited to attend an online assessment session (T1) in small groups, during which they provided informed consent and completed a battery of online measures (see below for a description of the measures). Prior to attending the online session, participants were instructed to situate themselves in a quiet room and turn on their video camera during the call, to monitor their environment and minimize external distractions in the background.
Study procedure
After completing the baseline measures, participants were informed of the condition they were assigned to. Participants assigned to the waitlist control group were informed that they would be invited to attend a T2 assessment approximately eight weeks later, following which they would receive an orientation to the online self-compassion program.
Meanwhile, participants in the intervention group received an orientation to the practice of self-compassion and the 29k mobile app, the platform through which the online self-compassion program was delivered, immediately after completing the T1 assessment. The orientation included an explanation of what self-compassion practice involves and how self-compassion can be helpful, as well as a clarification of common misconceptions about self-compassion. Participants were then given instructions on how to download and access the self-compassion program within the app.
Intervention program
The self-compassion program on the 29k app consisted of seven weekly lessons, each of which takes approximately 30 to 60 min to complete. Each lesson focused on a different theme related to self-compassion, such as “Inner critic”, “Shame”, and “Gratitude”.
To increase adherence, participants were instructed to block out a period of time each week where they would commit to watching the lessons and completing the associated self-compassion exercises. Additionally, participants were instructed to post written reflections on the exercises on Kudoboard, a platform that hosts anonymous discussion posts. This feature is an adaptation of the program’s original video call feature, which required participants to log on to the app at a pre-specified timing to share their reflections on the lessons. As there were technical issues associated with the video call feature, participants were instructed instead to post their reflections using the online discussion platform. Participants would be emailed a new link for each week’s Kudoboard, along with a few prompts specific to the lessons for that week. Example questions for reflections include: “How do you think finding an inner friend may help you when you’re feeling critical of yourself in the future?” Participants were also asked to read and reflect on each other’s reflections at the end of each week.
Eight weeks following T1 assessment, all participants were invited to attend the T2 assessment session. Participants were administered the same battery of measures that were administered at T1. For participants in the intervention group, they were asked to answer additional questions regarding their engagement with the app. These involved rating the app’s helpfulness and their satisfaction with the app, as well as providing general feedback on the self-compassion program.
After completing the T2 assessment, all participants received debriefing about the study. Participants in the waitlist control group were given an orientation to the 29k app at this time. All participants who completed the study were reimbursed via cash (SGD$15) or awarded research credits for their university course. Data collection for this study took place between November 2021 and January 2022.
Demographic questions
Participants were administered a list of demographic questions, including age, gender, ethnicity, marital status, nationality, and year of study. Participants were also assessed on their past experience engaging in self-compassion and mindfulness practices.
Depression, Anxiety, and Stress Scale (DASS-21)
The Depression, Anxiety and Stress Scale (DASS-21, Lovibond & Lovibond, 1995 ) is a 21-item scale that measures symptoms of depression, anxiety, and stress in the past week, which was used to measure participants’ level of psychological distress. This scale has previously been validated in a sample of Malaysian undergraduate students, with high internal consistencies of α = 0.85 to 0.91 (Ahmad et al., 2018 ). Items are rated on a 4-point Likert scale (0 = “Did not apply to me at all,” 1 = “Applied to me to some degree, or some of the time,” 2 = “Applied to me to a considerable degree or a good part of time,” 3 = “Applied to me very much or most of the time.”) Statements include “I found it hard to wind down,” “I felt I was close to panic,” and “I couldn’t seem to experience any positive feeling at all.” Internal consistency of the scale in the current sample was high at α = 0.89 for depression, α = 0.86 for anxiety, and α = 0.86 for stress.
Self-Compassion Scale (SCS)
Self-compassion was assessed using the 26-item Self-Compassion Scale (SCS; Neff, 2003b ). Items were rated on a five-point Likert type scale (1 = “almost never,” 5 = “almost always.”), and the items assess six components of self-compassion: self-kindness, self-judgment, common humanity, isolation, mindfulness, and over-identification. A sample item is “I try to be loving towards myself when I’m feeling emotional pain.” The scale was found to have high internal consistency in a sample of undergraduate students (Neff, 2003b ). In the current sample, the scale’s internal consistency is excellent (α = 0.93).
Perceptions of Academic Stress (PAS) Scale
Academic worry was measured using the Perceptions of Academic Stress Scale (PAS; Bedewy & Gabriel, 2015 ). The scale consists of 18 items that measure several aspects of academic worry, namely: pressures to perform, perceptions of workload, academic self-perceptions, and time restraints. A sample item is “The competition with my peers for grades is quite intense.” The scale has been validated in an undergraduate sample and demonstrated good internal consistency (Bedewy & Gabriel, 2015 ). The scale’s internal consistency is high (α = 0.86) in the current sample.
Almost Perfect Scale Revised (APS-R)
An adapted version of the Almost Perfect Scale Revised (APS-R, Slaney et al., 2001 ) was administered to measure perfectionism. The revised scale was validated in an undergraduate sample, with internal consistencies of each subscale and the overall scale ranging from α = 0.82 to 0.92 (Slaney et al., 2001 ). Two of the subscales, discrepancy and high standards, were used to measure perfectionism. The discrepancy subscale consists of 12 items and measures the construct of discrepancies between one’s expectations of oneself and one’s actual performance, while the high standards subscale consists of 7 items and measures the construct of setting high standards for oneself. The resulting scale is a 19-item, 7-point Likert scale (1= “Strongly Disagree,” 7 = “Strongly Agree”), and participants were asked to rate their agreement with statements such as “I am seldom able to meet my own high standards of performance.” Internal consistency of the adapted scale was excellent at α = 0.94 in the current sample.
Rumination Response Scale (RRS)
The Rumination Response Scale (RRS, Nolen-Hoeksema & Morrow, 1991 ) was administered to assess participants’ level of rumination. This scale consists of 22 items and was validated in a sample of U.S. adults, with an internal consistency of α = 0.90 and test-retest correlation coefficient of 0.67. Participants were asked to rate how often they identified with each statement on a four-point Likert type scale (1 = “almost never,” 4 = “almost always.”). Sample items include “I think about how sad I feel.” In the current sample, the scale’s internal consistency was excellent (α = 0.93).
Marlowe-Crowne Social Desirability Scale
A short form of the Marlowe-Crowne Social Desirability Scale (Reynolds, 1982 ) was administered to assess whether social desirability was a predictor of change in the outcome measures. The measure is a 13-item scale that measures individuals’ tendencies to provide socially desirable responses. This scale has been validated in an undergraduate sample, with good reliability and validity (Reynolds, 1982 ). Participants selected “True” or “False” in response to a number of statements, such as “I’m always willing to admit to it when I make a mistake.” This measure was administered at T1 assessment only, to assess whether social desirability would predict changes in the outcome measures. Internal consistency of the scale was acceptable at α = 0.66 in the current sample.
29k App Experience
Participants in the intervention group were administered additional questions at T2 regarding their experience with the 29k app. Specifically, they were asked to indicate the number of weeks for which they completed the lessons, wrote their own reflections on Kudoboard, and read others’ reflections on Kudoboard. They were also asked to rate, on a Likert scale of 1 to 7, how helpful they found the app to be (1 = “Not helpful at all,” 7 = “Very helpful,”) as well as how satisfied they were with the app (1 = “Not satisfied at all,” 7 = “Very satisfied.”) Lastly, they were asked to provide open-ended feedback on their experiences with the app.
Data Analytic Plan
The data was analyzed using Statistical Package for the Social Sciences (SPSS). In the preliminary analyses, the data was checked for normality and outliers were excluded. To check whether randomization was successful, the two conditions were tested for equivalence at T1. Chi-square tests were conducted to assess whether participants across conditions differed in proportion of gender, ethnicity, marital status, nationality, prior self-compassion experience, or prior mindfulness experience. Independent samples t -tests were also conducted to examine whether there were between-condition differences on age, social desirability, or any of the dependent variables. All demographic variables, prior self-compassion experience, prior mindfulness experience, and social desirability were assessed as potential covariates, using a hierarchical linear regression approach. In each analysis, T2 scores of each dependent variable were regressed on the corresponding T1 score, with the potential covariate entered in the second step. If significant covariates were identified, they were subsequently controlled for in the main analyses. In the main analyses, a 2 × 2 mixed analysis of variance (ANOVA) was run to examine the effects of experimental condition on changes in each of the dependent variables from T1 to T2, with Time (T1 vs. T2) as the within-subject factor, and Condition (intervention vs. waitlist control) as the between-subject factor. Feasibility of the intervention was assessed by calculating the rate of completion (with completion of the intervention being defined as having completed a minimum of five out of seven sessions) and overall number of sessions completed. Feedback on the 29k app was qualitatively analyzed using Elo and Kyngäs ( 2008 )’s guidelines.
Sample characteristics
Of all participants who enrolled in the study, six participants from the intervention condition and four participants from the waitlist control condition dropped out of the study and did not complete the T2 assessments. Their data were excluded from later analyses. Table 1 presents a summary of participants’ demographic information. Participants were 21.2 years old on average ( SD = 1.96, range = 18 to 27). More than half were female participants (64.2%). The majority of participants identified as Chinese (71.1%), while the rest identified as Malay, Indian, or other ethnicities. Most participants identified as Singaporean (73.6%) and single (69.8%). Almost all participants were undergraduate students (98.1%). Most participants reported not having any prior self-compassion experience (94.3%) or prior mindfulness experience (92.5%).
Preliminary analyses
Randomization check.
At baseline, both conditions did not differ on gender, ethnicity, marital status, nationality, prior self-compassion, prior mindfulness experience, social desirability, academic worry, perfectionism, anxiety, or stress, p s > 0.05. Results from independent samples t -tests indicated that compared to the waitlist control group, the intervention group scored significantly lower on self-compassion, F (1, 51) = 1.79, p = .012, 95% CI [−0.82, −0.10], and higher on rumination, F (1, 51) = 0.46, p = .007, 95% CI [3.16, 18.52], and depression, F (1, 51) = 0.52, p = .025, 95% CI [0.47, 6.66], at T1. These variables were subsequently assessed as potential covariates to examine if they predicted changes in outcome variables from T1 to T2. Table 2 presents independent samples t -test statistics.
Covariate analyses
To determine whether any demographic variables (gender, ethnicity, marital status, nationality), background variables (prior self-compassion, prior mindfulness experience, social desirability), or differences in baseline scores (T1 trait self-compassion, T1 rumination, T1 depression) predicted changes on any of the dependent variables, a series of multiple linear regressions were run. It was found that seven regression models were significant. The analyses showed that changes in trait self-compassion were predicted by T1 rumination, t = 4.11, p < .001, 95% CI [0.007, 0.022], and T1 depression, t = 2.46, p = .017, 95% CI [0.004, 0.042]. Changes in rumination were predicted by T1 depression, t = 2.61, p = .012, 95% CI [0.19, 1.48], and changes in perfectionism were predicted by prior self-compassion experience, t = 2.05, p = .045, 95% CI [0.45, 40.00], T1 rumination scores, t = 2.49, p = .016, 95% CI [0.083, 0.77], and T1 depression scores, t = 2.03, p = .048, 95% CI [0.010, 1.79]. Lastly, prior self-compassion experience was a significant predictor of changes in stress, t = 2.82, p = .007, 95% CI [1.89, 11.3]. Subsequently, these variables were incorporated into the main analyses as covariates.
Primary analyses
A mixed ANOVA was used to determine the interaction effects for Time (T1 vs. T2) × Condition (intervention vs. waitlist control), after controlling for covariates that were identified earlier. Table 3 presents the descriptive statistics and inferential statistics for the analyses. As the effects pertinent to our hypotheses were the Time × Condition effects, we focused primarily on reporting these effects in text. Statistics regarding the main effects of Time and Conditions for each variable respectively is presented in the table.
For depression, there was a significant Time × Condition interaction effect, F (1, 51) = 7.27, p = .009. Compared to participants in the control group, participants in the intervention condition reported significantly greater decreases in depressive symptoms. There was a trend for a main effect of Time, F (1, 51) = 2.93, p = .093, indicating that on average, participants across both conditions reported reduced symptoms of depression over time. For anxiety, there was also a significant Time × Condition effect, F (1, 51) = 7.45, p = .009, with participants in the intervention condition reporting greater decreases in anxiety compared to those in the control condition, and a non-significant effect of Time, F (1, 51) = 1.94, p = .170. For stress, there was a significant interaction effect, F (1, 51) = 4.24, p = .045, indicating that participants in the intervention group reported greater decreases in stress compared to participants in the control group. There was also a significant effect of Time, F (1, 51) = 10.45, p = .002, indicating that participants reported decreases in stress on average, over time.
For trait self-compassion, there was a significant effect of Time, F (1, 51) = 17.14, p < .001, and a non-significant Time x Condition effect, F (1, 51) = 0.38, p = .539. Participants reported significantly increased self-compassion from T1 to T2, regardless of the condition they were assigned to. For academic worry, there was a marginally significant Time x Condition interaction effect, F (1, 51) = 3.43, p = .070, and a non-significant effect of Time, F (1, 51) = 0.02, p = .877. Participants in the intervention group reported a trend towards greater decreases in academic worry over time compared to participants in the control group. For both rumination and perfectionism, there were no significant effects of either Time or Time × Condition interaction.
Adherence to intervention
On average, participants assigned to the self-compassion program completed 6.20 lessons ( SD = 1.41) out of 7 sessions. Most participants completed at least five out of seven lessons ( n = 23; 92%). Relative to the self-compassion lessons, participants were less engaged with the Kudoboard reflections. On average, participants wrote their own reflections for 4.80 out of 7 weeks ( SD = 2.42), and read others’ reflections in 3.88 out of 7 weeks ( SD = 2.09).
App feedback
Of the 25 participants who underwent the intervention, all but one (96% response rate) completed an open-ended feedback question on the 29k app after the study. The results are summarized in Table 4 . Majority of the participants gave positive feedback for the app’s features. Four participants (16%) highlighted that the app increased their accessibility to self-compassion techniques, and three participants (12%) indicated that the app interface was intuitive and easy to use. In contrast, three participants (12%) found the app interface difficult to navigate and not sufficiently user-friendly.
Generally, many participants also reported positive feedback about the course content. Consistent with the quantitative findings, three participants (12%) reported that the program has helped them to grow and learn to be more self-compassionate. Five participants (20%) reported feeling that the course was well-structured; two participants (8%) expressed appreciation for the introspective exercises; and another two participants (8%) reported enjoying the trainer’s relatable shared experiences. There were also areas that participants felt could be improved in terms of course content. Two participants (8%) noted that the video lessons were too long, with another two participants (8%) finding the videos inconsistent in their engagement. Six participants (25%) found the course content to be unrelatable in some aspects, and three participants (12%) reported feeling that the course would not result in long-term changes for them.
Participants in the intervention group were also asked to rate the app’s helpfulness and their satisfaction with the app. On a 1-to-7 Likert scale (1 = least helpful; 7 = most helpful), participants’ average rating for the app’s helpfulness was 4.20 ( SD = 1.50). In terms of the level of satisfaction with the app, participants reported an average rating of 4.44 ( SD = 1.36) on the 7-point scale.
The present study examined the effects of a seven-week app-based self-compassion program on psychological health outcomes, in a sample of college students based in Singapore. Results showed that relative to the waitlist control condition, participants of the self-compassion program demonstrated significant decreases in depression, anxiety, and stress from pre- to post-intervention. There was also a trend for greater decreases in academic worry among participants in the self-compassion program compared to the control group participants. Contrary to prediction, no between-group differences were found on changes in perfectionism and rumination.
The finding that the self-compassion-based phone app led to significant improvements in depressive symptoms, anxiety, and stress is consistent with past research demonstrating that self-compassion-based interventions are effective in improving psychological health outcomes (Ferrari et al., 2019 ). Specifically, the findings suggest that attending the app-based MSC program may be effective in alleviating psychological symptoms. The current finding adds to the literature by demonstrating that phone apps are an effective platform to support the delivery of self-compassion-based interventions, with beneficial mental health outcomes.
Contrary to expectation, usage of the app did not lead to differentially greater increases in trait self-compassion in the intervention group compared to the control group. This finding could be attributed to the fact that the program implemented in this study was delivered via a phone app without a live facilitator, in contrast to past studies that delivered self-compassion interventions via live teaching and/or in-person engagements (Ferrari et al., 2019 ). Without specific guidance and support, participants may have found it more challenging to internalize the self-compassion messaging from the app. A hybrid intervention format, incorporating real-time human interaction with trained facilitators through the app, could potentially be more effective in helping participants develop self-compassion. A study by Campion and Glover ( 2016 ), involving a series of semi-structured interviews with non-clinical participants following brief engagement in a self-compassion meditation practice, revealed a concern that practising self-compassion may be viewed as a form of vulnerability in society. Further understanding of the barriers to practicing self-compassion is necessary for creating more effective interventions targeting a college population. Notably however, the current study found that averaging across conditions, participants reported significant increases in self-compassion from pre- to post-intervention. It remains to be examined whether mere exposure to the concept of self-compassion, or a desire to become more self-compassionate as evidenced by participants’ initiative in signing up for the self-compassion program, may have naturally led to increases in trait self-compassion among participants assigned to the control condition.
Meanwhile, the study found a trend for participants in the self-compassion intervention to report lower levels of academic worry post-intervention compared to control group participants. This finding is consistent with other studies demonstrating positive effects of self-compassion interventions on anxiety (Ferrari et al., 2019 ; Woodfin et al., 2021 ). Notably however, the effect size is small, which may be explained by a lack of specificity in the 29k program in targeting academic worry, or academic-related stress. Analyses of qualitative feedback revealed that a number of participants ( n = 6) found the content of the app “hard to identify with,” “not very relatable,” or expressed that they were “disengaged from the material”. It remains to be investigated whether tailoring the content of the intervention for college students would yield stronger effects with regards to addressing academic worry. It is also plausible that the effects of the intervention on academic worry may emerge more strongly among participants with higher baseline academic worry, as suggested by a study that found significant decreases in assessment anxiety following a compassionate imagery intervention, only among college students with high levels of assessment anxiety at baseline (McEwan et al., 2018 ).
The finding that participation in the 29k app program did not result in greater decreases in rumination and perfectionism among intervention participants contradicts findings of past studies, which showed that self-compassion interventions lead to reductions in rumination (Ferrari et al., 2019 ), and both adaptive and maladaptive perfectionism (Woodfin et al., 2021 ). The lack of significant reduction in these variables could be attributed to the fact that the present study delivered the intervention primarily using pre-recorded content on a phone app, which may have reduced the efficacy of the intervention in addressing maladaptive cognitive processes. Incorporation of live teaching and experiential exercises may increase participant engagement and consolidate learning in terms of disrupting habitual cognitive and dispositional tendencies. Further, delivery of intervention in an individual, self-paced format may be less effective than a group format, as demonstrated by a meta-analysis assessing the effects of self-compassion-based interventions on psychological health outcomes (Ferrari et al., 2019 ). Interestingly, despite a lack of effect on rumination and perfectionism, the intervention led to differential improvements in depression, anxiety, and stress, suggesting that alternative mechanisms (e.g., proactive coping) may underlie the effects of the intervention on psychological health (Huang et al., 2021 ).
With regards to the feasibility and acceptability of the intervention, the study found that the 29k program was feasible and acceptable, as indicated by a high overall completion rate (92%). Overall, participants reported moderate levels of satisfaction with the program. In the open feedback given during T2 assessments, a number of participants reported that the program helped them develop self-compassion, whereas others highlighted that they experienced difficulties when completing the course. Examples of these comments were that some of the lessons felt forced or unhelpful, that the lessons adopted an unrealistically positive outlook, or that it was challenging to internalize the app’s teachings. Despite the feedback, quantitative analyses demonstrated that there were notable improvements in participants’ overall psychological health. Future research could examine whether systematic adaptations of the app’s content to suit college students’ context and stressors could improve the intervention’s acceptability and efficacy. Further, as highlighted earlier, adding live coaching and/or teaching sessions could potentially enhance the intervention’s engagement of participants and consolidate learning.
In terms of the study’s strengths, use of a randomized controlled trial design enables causal conclusions to be drawn regarding the effects of the intervention. Notably however, the experimental conditions differed at baseline on several outcome variables, and efforts were made to assess whether these variables predicted changes in the other outcome variables and therefore needed to be controlled for. Nonetheless, we cannot rule out the possibility that some of the findings may have been influenced by pre-existing baseline differences between the experimental conditions. Assessing the potential role of social desirability in predicting changes in the outcome variables enabled us to rule out social desirability bias as a factor that may confound the findings. Examining use of a mobile app in the delivery of the intervention was timely given that the spread of the COVID-19 pandemic limited individuals’ access to mental health professionals (Keshavan, 2020 ), and the app offered an alternative platform for students who may be struggling with psychological distress to access mental healthcare resources. Importantly, the findings add to the literature pertaining to the effects of self-compassion interventions in the Southeast Asian cultural context.
With regards to limitations, the study’s analyzed sample size ( n = 53) is smaller than the number derived from power analyses. This resulted from participant attrition, as a number of participants dropped out of the study due to a busy schedule and inability to commit time to complete the intervention. It should be noted meanwhile that the dropout rate (15.9%) is lower than averaged dropout rates reported in other studies involving delivery of interventions using mobile apps (e.g., 24%; Linardon, 2023 ). Further, participation in the Kudoboard reflection activities varied significantly among participants, potentially due to the activities being delivered asynchronously on a platform separate from the app. Future studies may examine other means for sharing of experiences within the group, such as creating an interactive group chat where participants could respond to each other’s reflections in real time, or scheduling online group meetings with a trained facilitator. This may also reduce attrition, by allowing participants to feel a greater sense of connectedness with other participants in the group. Incorporation of an active control group would also enable us to assess the unique effects of the self-compassion-intervention program over and above placebo effects. Further, we did not assess the extent to which participants engaged in home self-compassion practices outside of the app program. Future research could examine the extent to which the amount or frequency of home practice predicts improvements resulting from participating in the self-compassion program. Lastly, it should be noted that the app contains programs other than the adapted MSC program. While participants were explicitly instructed to access only the adapted MSC program in the study, we were not able to track whether any participant had accessed the other programs during their participation in the study.
In summary, the present study found that an adaptation of the MSC program delivered via a mobile app, 29k , was effective at reducing symptoms of depression, anxiety, and stress in a college student sample. These results are promising and point to the potential for the app to be more widely implemented in the student population. This is particularly important in times when there is a pandemic, as there tends to be heightened stress and uncertainty amongst students. Compared to in-person mental health services, mobile apps afford the advantages of being more cost-effective and accessible, and may be more sought after by students unwilling to seek out mental health professionals due to stigma-related concerns (Levin et al., 2018 ). Future research should examine whether alternative forms of delivering the intervention (e.g., incorporating live teaching and adapting the content for college students) would enhance the program’s effectiveness in increasing trait self-compassion and reducing maladaptive cognitive traits. Future work could also investigate the effects of longer-term engagement in self-compassion practices among college students, and whether the benefits would translate into other domains such as quality of life, academic performance, and interpersonal relationships.
Data availability
The dataset analyzed in the current study is available in the Open Science Framework data repository, https://osf.io/9t4ws/ .
Ahmad, N., Roslan, S., Othman, S., Shukor, S. F. A., & Bakar, A. Y. A. (2018). The validity and reliability of psychometric profile for Depression, anxiety and stress scale (DASS21) instrument among Malaysian undergraduate students. International Journal of Academic Research in Business and Social Sciences , 8 (6), 812–827. https://doi.org/10.6007/IJARBSS/v8-i6/4275
Article Google Scholar
Al-Refae, M., Al-Refar, A., Munroe, M., Sardella, N. A., & Ferrari, M. (2021). A self-compassion and mindfulness-based cognitive mobile intervention (serene) for depression, anxiety and stress: Promoting adaptive emotional regulation and wisdom. Frontiers in Psychology , 12 , 648087. https://doi.org/10.3389/fpsyg.2021.648087
Article PubMed PubMed Central Google Scholar
Andersson, C., Bergsten, K. L., Lilliengren, P., Norbäck, K., Rask, K., Einhorn, S., & Osika, W. (2021). The effectiveness of smartphone compassion training on stress among Swedish university students: A pilot randomized trial. Journal of Clinical Psychology , 77 (4), 927–945. https://doi.org/10.1002/jclp.23092
Article PubMed Google Scholar
Ang, R. P., Klassen, R. M., Chong, W. H., Huan, V. S., Wong, I. Y. F., Yeo, L. S., & Krawchuk, L. L. (2009). Cross-cultural invariance of the academic expectations stress inventory: Adolescent samples from Canada and Singapore. Journal of Adolescence , 32 (5), 1225–1237. https://doi.org/10.1016/j.adolescence.2009.01.009
Bedewy, D., & Gabriel, A. (2015). Examining perceptions of academic stress and its sources among university students: The perception of academic stress scale. Health Psychology Open , 2 (2). https://doi.org/10.1177/2055102915596714
Begin, C., Berthod, J., Martinez, L. Z., & Truchon, M. (2022). Use of mobile apps and online programs of mindfulness and self-compassion training in workers: A scoping review. Journal of Technology and Behavioral Science , 7 , 477–515. https://doi.org/10.1007/s41347-022-00267-1
Beiter, R., Nash, R., McCrady, M., Rhoades, D., Linscomb, M., Clarahan, M., & Sammut, S. (2015). The prevalence and correlates of depression, anxiety, and stress in a sample of college students. Journal of Affective Disorders , 173 , 90–96. https://doi.org/10.1016/j.jad.2014.10.054
Birmingham, W. C., Wadsworth, L. L., Lassetter, J. H., Graff, T. C., Lauren, E., & Hung, M. (2021). COVID-19 lockdown: Impact on college students’ lives. Journal of American College Health , 1–15. https://doi.org/10.1080/07448481.2021.1909041
Campion, M., & Glover, L. (2016). A qualitative exploration of responses to self-compassion in a non-clinical sample. Health & Social Care in the Community, 25 (3), 1100–1108. https://doi.org/10.1111/hsc.12408
Clabaugh, A., Duque, J., & Fields, L. (2021). Academic stress and emotional well-being in United States college students following onset of the COVID-19 pandemic. Frontiers in Psychology , 12 . https://doi.org/10.3389/fpsyg.2021.628787
Dobos, B., Piko, B. F., & Mellor, D. (2021). What makes university students perfectionists? The role of childhood trauma, emotional dysregulation, academic anxiety, and social support. Scandinavian Journal of Psychology , 62 (3), 443–447. https://doi.org/10.1111/sjop.12718
Egan, S. J., Wade, T. D., & Shafran, R. (2011). Perfectionism as a transdiagnostic process: A clinical review. Clinical Psychology Review , 31 (2), 203–212. https://doi.org/10.1016/j.cpr.2010.04.009
Elo, S., & Kyngäs, H. (2008). The qualitative content analysis process. Advanced Nursing , 62 (1), 107–115. https://doi.org/10.1111/j.1365-2648.2007.04569.x
Eum, K., & Rice, K. G. (2011). Test anxiety, perfectionism, goal orientation, and academic performance. Anxiety Stress & Coping , 24 (2), 167–178. https://doi.org/10.1080/10615806.2010.488723
Faul, F., Erdfelder, E., Lang, A. G., & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods , 39 (2), 175–191. https://doi.org/10.3758/BF03193146
Ferrari, M., Hunt, C., Harrysunker, A., Abbott, M. J., Beath, A. P., & Einstein, D. A. (2019). Self-compassion interventions and psychosocial outcomes: A meta-analysis of RCTs. Mindfulness , 10 (8), 1455–1473. https://doi.org/10.1007/s12671-019-01134-6
Finlay-Jones, A., Kane, R., & Rees, C. (2017). Self-compassion online: A pilot study of an internet-based self-compassion cultivation program for psychology trainees. Journal of Clinical Psychology , 73 (7), 797–816. https://doi.org/10.1002/jclp.22375
Huang, J., Nigatu, Y. T., Smail-Crevier, R., Zhang, X., & Wang, J. (2018). Interventions for common mental health problems among university and college students: A systematic review and meta-analysis of randomized controlled trials. Journal of Psychiatric Research , 107 , 1–10. https://doi.org/10.1016/j.jpsychires.2018.09.018
Huang, J., Lin, K., Fan, L., Qiao, S., & Wang, Y. (2021). The effects of a self-compassion intervention on future-oriented coping and psychological well-being: A randomized controlled trial in Chinese college students. Mindfulness , 12 (6), 1451–1458. https://doi.org/10.1007/s12671-021-01614-8
Hurst, C. S., Baranik, L. E., & Daniel, F. (2013). College student stressors: A review of the qualitative research. Stress and Health: Journal of the International Society for the Investigation of Stress , 29 (4), 275–285. https://doi.org/10.1002/smi.2465
Keshavan, M. S. (2020). Pandemics and psychiatry: Repositioning research in context of COVID-19. Asian Journal of Psychiatry , 51 , 102–159. https://doi.org/10.1016/j.ajp.2020.102159
Krieger, T., Martig, D. S., van den Brink, E., & Berger, T. (2016). Working on self-compassion online: A proof of concept and feasibility study. Internet Interventions , 6 , 64–70. https://doi.org/10.1016/j.invent.2016.10.001
Lee, K. J., & Lee, S. M. (2022). The role of self-compassion in the academic stress model. Current Psychology , 41 , 3195–3204. https://doi.org/10.1007/s12144-020-00843-9
Levin, M. E., Krafft, J., & Levin, C. (2018). Does self-help increase rates of help seeking for student mental health problems by minimizing stigma as a barrier? Journal of American College Health , 66 (4), 302–309. https://doi.org/10.1080/07448481.2018.1440580
Li, Y., Wang, A., Wu, Y., Han, N., & Huang, H. (2021). Impact of the COVID-19 pandemic on the mental health of college students: A systematic review and meta-analysis. Frontiers in Psychology , 12 , 669119. https://doi.org/10.3389/fpsyg.2021.669119
Limburg, K., Watson, H. J., Hagger, M. S., & Egan, S. J. (2017). The relationship between perfectionism and psychopathology: A meta-analysis. Journal of Clinical Psychology , 73 (10), 1301–1326. https://doi.org/10.1002/jclp.22435
Linardon, J. (2020). Can acceptance, mindfulness, and self-compassion be learned by smartphone apps? A systematic and meta-analytic review of randomized controlled trials. Behavior Therapy , 51 (4), 646–658. https://doi.org/10.1016/j.beth.2019.10.002
Linardon, J. (2023). Rates of attrition and engagement in randomized controlled trials of mindfulness apps: Systematic review and meta-analysis. Behaviour Research and Therapy , 170 , Article 104421. https://doi.org/10.1016/j.brat.2023.104421
Lovibond, S. H., & Lovibond, P. F. (1995). Manual for the depression anxiety stress scales (2nd ed.). Psychology Foundation.
Google Scholar
Luca, M. (2019). Maladaptive rumination as a transdiagnostic mediator of vulnerability and outcome in psychopathology. Journal of Clinical Medicine , 8 (3), 314. https://doi.org/10.3390/jcm8030314
MacBeth, A., & Gumley, A. (2012). Exploring compassion: A meta-analysis of the association between self-compassion and psychopathology. Clinical Psychology Review , 32 (6), 545–552. https://doi.org/10.1016/j.cpr.2012.06.003
McEwan, K., Elander, J., & Gilbert, P. (2018). Evaluation of a web-based self-compassion intervention to reduce student assessment anxiety. Interdisciplinary Education and Psychology , 2 (1), 1–24. https://doi.org/10.31532/InterdiscipEducPsychol.2.1.006
McLaughlin, K. A., & Nolen-Hoeksema, S. (2011). Rumination as a transdiagnostic factor in depression and anxiety. Behaviour Research and Therapy , 49 (3), 186–193. https://doi.org/10.1016/j.brat.2010.12.006
Moawad, R. (2020). Online learning during the COVID-19 pandemic and academic stress in university students. Revista Romaneasca Pentru Educatie Multidimensionala , 12 (1), 100–107. https://doi.org/10.18662/rrem/12.1sup2
Nambiar, D. (2020). The impact of online learning during COVID-19: Students’ and teachers’ perspective. The International Journal of Indian Psychology , 8 (2), 783–793. https://doi.org/10.25215/0802.094
Neff, K. D. (2003a). Self-compassion: An alternative conceptualization of a healthy attitude toward oneself. Self and Identity , 2 (2), 85–101. https://doi.org/10.1080/15298860309032
Neff, K. D. (2003b). The development and validation of a scale to measure self-compassion. Self and Identity , 2 , 223–250. https://doi.org/10.1080/15298860390209035
Neff, K. D., & Germer, C. K. (2013). A pilot study and randomized controlled trial of the mindful self-compassion program. Journal of Clinical Psychology , 69 (1), 28–44. https://doi.org/10.1002/jclp.21923
Nolen-Hoeksema, S. (2000). The role of rumination in depressive disorders and mixed anxiety/depressive symptoms. Journal of Abnormal Psychology , 109 (3), 504–511. https://doi.org/10.1037/0021-843X.109.3.504
Nolen-Hoeksema, S., & Morrow, J. (1991). A prospective study of depression and posttraumatic stress symptoms after a natural disaster: The 1989 Loma Prieta earthquake. Journal of Personality and Social Psychology , 61 (1), 115–121. https://doi.org/10.1037/0022-3514.61.1.115
Poh, B. (2018, September 29). Commentary: A hyper-competitive culture is breeding severe test anxiety among many students . CNA. Retrieved Feb 2, 2024 from https://www.channelnewsasia.com/commentary/hyper-competitive-culture-breeding-severe-test-anxiety-among-799076
Rauschenberg, C., Schick, A., Goetzl, C., Roehr, S., Riedel-Heller, S. G., Koppe, G., Durstewitz, D., Krumm, S., & Reininghaus, U. (2021). Social isolation, mental health, and use of digital interventions in youth during the COVID-19 pandemic: A nationally representative survey. European Psychiatry: The Journal of the Association of European Psychiatrists , 64 (1), e20. https://doi.org/10.1192/j.eurpsy.2021.17
Reynolds, W. M. (1982). Development of reliable and valid short forms of the Marlowe-Crowne Social Desirability Scale. Journal of Clinical Psychology , 38 (1), 119–125. https://doi.org/10.1002/1097-4679(198201)38:1%3C;119::AID-JCLP2270380118%3E3.0.CO;2-I
Richardson, C. M. E., Trusty, W. T., & George, K. A. (2020). Trainee wellness: Self-critical perfectionism, self-compassion, depression, and burnout among doctoral trainees in psychology. Counselling Psychology Quarterly , 33 (2), 187–198. https://doi.org/10.1080/09515070.2018.1509839
Rodriguez-Villa, E., Naslund, J., Keshavan, M., Patel, V., & Torous, J. (2020). Making mental health more accessible in light of COVID-19: Scalable digital health with digital navigators in low and middle-income countries. Asian Journal of Psychiatry , 54 , 102433. https://doi.org/10.1016/j.ajp.2020.102433
Samaie, G., & Farahani, H. A. (2011). Self-compassion as a moderator of the relationship between rumination, self-reflection and stress. Procedia - Social and Behavioral Sciences , 30 , 978–982. https://doi.org/10.1016/j.sbspro.2011.10.190
Sheldon, E., Simmonds-Buckley, M., Bone, C., Mascarenhas, T., Chan, N., Wincott, M., Gleeson, H., Sow, K., Hind, D., & Barkham, M. (2021). Prevalence and risk factors for mental health problems in university undergraduate students: A systematic review with meta-analysis. Journal of Affective Disorders , 287 , 282–292. https://doi.org/10.1016/j.jad.2021.03.054
Slaney, R. B., Rice, K. G., Mobley, M., Trippi, J., & Ashby, J. S. (2001). The revised almost perfect scale. Measurement and Evaluation in Counselling and Development , 34 , 130–145. https://doi.org/10.1080/07481756.2002.12069030
Smeets, E., Neff, K., Alberts, H., & Peters, M. (2014). Meeting suffering with kindness: Effects of a brief self-compassion intervention for female college students. Journal of Clinical Psychology , 70 (9), 794–807. https://doi.org/10.1002/jclp.22076
Stoeber, J., Lalova, A. V., & Lumley, E. J. (2020). Perfectionism, (self-)compassion, and subjective well-being: A mediation model. Personality and Individual Differences , 154 , 109708. https://doi.org/10.1016/j.paid.2019.109708
Treynor, W., Gonzalez, R., & Nolen-Hoeksema, S. (2003). Rumination reconsidered: A psychometric analysis. Cognitive Therapy and Research , 27 , 247–259. https://doi.org/10.1023/A:1023910315561
Wang, C., Wen, W., Zhang, H., Ni, J., Jiang, J., Cheng, Y., Zhou, M., Ye, L., Feng, Z., Ge, Z., Luo, H., Wang, M., Zhang, X., & Liu, W. (2021). Anxiety, depression, and stress prevalence among college students during the COVID-19 pandemic: A systematic review and meta-analysis. Journal of American College Health , 71 (7), 2123–2130. https://doi.org/10.1080/07448481.2021.1960849
Williams, J. G., Stark, S. K., & Foster, E. E. (2008). Start today or the very last day? The relationships among self-compassion, motivation, and procrastination. American Journal of Psychological Research , 4 (1), 37–44.
Woodfin, V., Molde, H., Dundas, I., & Binder, P. E. (2021). A randomized control trial of a brief self-compassion intervention for perfectionism, anxiety, depression, and body image. Frontiers in Psychology , 12 , 751294. https://doi.org/10.3389/fpsyg.2021.751294
Zessin, U., Dickhäuser, O., & Garbade, S. (2015). the relationship between self-compassion and well-being: A meta-analysis. Applied Psychology Health and Well-being , 7 (3), 340–364. https://doi.org/10.1111/aphw.12051
Download references
Open Access funding enabled and organized by CAUL and its Member Institutions. This study was funded by Yale-NUS College.
Author information
Authors and affiliations.
Division of Social Sciences, Yale-NUS College, Singapore, Singapore
Wei Tian Han, Karen Pooh, Ziying Wang & Madhumitha Ayyappan
Department of Psychology, School of Medical and Life Sciences, Sunway University, Petaling Jaya, Malaysia
Shian-Ling Keng
Department of Psychology, Monash University Malaysia, Subang Jaya, Malaysia
You can also search for this author in PubMed Google Scholar
Contributions
WTH, SLK, and KP conceptualized the study. WTH executed the study, led data collection and analyses, and drafted the manuscript. SLK and KP edited the manuscript. ZW and MA assisted with data collection and analysis of qualitative data. All authors reviewed and approved the manuscript prior to submission.
Corresponding author
Correspondence to Shian-Ling Keng .
Ethics declarations
This study was reviewed and approved by the institution’s Undergraduate Research Ethics Committee. The procedures in the study were performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Consent to participate
All participants gave their informed consent prior to their inclusion in the study. Participants signed informed consent regarding publishing their data.
Competing interests
The authors declare that they have no relevant financial or non-financial interests to disclose.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ .
Reprints and permissions
About this article
Han, W.T., Keng, SL., Pooh, K. et al. Effects of a mobile-app-based self-compassion intervention on psychological health and maladaptive cognitive traits: findings from a randomized controlled trial. Curr Psychol (2024). https://doi.org/10.1007/s12144-024-06441-3
Download citation
Accepted : 18 July 2024
Published : 20 August 2024
DOI : https://doi.org/10.1007/s12144-024-06441-3
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Self-compassion
- Academic worry
- College students
- App-based interventions
- Mental health
- Find a journal
- Publish with us
- Track your research
- Open access
- Published: 21 August 2024
Has cross-level clinical coordination changed in the context of the pandemic? The case of the Catalan health system
- Daniela Campaz-Landazabal ORCID: orcid.org/0000-0002-3211-960X 1 ,
- Ingrid Vargas ORCID: orcid.org/0000-0002-1778-2411 1 ,
- Elvira Sánchez ORCID: orcid.org/0000-0003-2549-322X 2 ,
- Francesc Cots ORCID: orcid.org/0000-0003-0238-8902 3 ,
- Pere Plaja ORCID: orcid.org/0000-0001-9488-8626 4 ,
- Joan Manuel Perez-Castejón ORCID: orcid.org/0000-0003-2618-8040 5 ,
- Antonio Sánchez-Hidalgo 6 &
- María Luisa Vázquez ORCID: orcid.org/0000-0002-6091-8193 1
BMC Health Services Research volume 24 , Article number: 959 ( 2024 ) Cite this article
Metrics details
The COVID-19 pandemic triggered numerous changes in health services organisation, whose effects on clinical coordination are unknown. The aim is to analyse changes in the experience and perception of cross-level clinical coordination and related factors of primary (PC) and secondary care (SC) doctors in the Catalan health system between 2017 and 2022.
Comparison of two cross-sectional studies based on online surveys by means of the self-administration of the COORDENA-CAT (2017) and COORDENA-TICs (2022) questionnaires to PC and SC doctors. Final sample n = 3308 in 2017 and n = 2277 in 2022. Outcome variables: experience of cross-level information and clinical management coordination and perception of cross-level clinical coordination in the healthcare area and related factors. Stratification variables: level of care and year. Adjusting variables: sex, years of experience, type of specialty, type of hospital, type of management of PC/SC. Descriptive bivariate and multivariate analysis using Poisson regressions models to detect changes between years in total and by levels of care.
Compared with 2017, while cross-level clinical information coordination remained relatively high, with a slight improvement, doctors of both care levels reported a worse experience of cross-level clinical management coordination, particularly of care consistency (repetition of test) and accessibility to PC and, of general perception, which was worse in SC doctors. There was also a worsening in organisational (institutional support, set objectives, time available for coordination), attitudinal (job satisfaction) and interactional factors (knowledge between doctors). The use of ICT-based coordination mechanisms such as shared electronic medical records and electronic consultations between PC and SC increased, while the participation in virtual joint clinical conferences was limited.
Conclusions
Results show a slight improvement in clinical information but also less expected setbacks in some dimensions of clinical management coordination and in the perception of clinical coordination, suggesting that the increased use of some ICT-based coordination mechanisms did not counteract the effect of the worsened organisational, interactional, and attitudinal factors during the pandemic. Strategies are needed to facilitate direct communication, to improve conditions for the effective use of mechanisms and policies to protect healthcare professionals and services in order to better cope with new crises.
Peer Review reports
Introduction
Cross-level clinical coordination is a priority for health systems, particularly for national health systems (NHS) based on primary care (PC), such as the Catalan health system, as it contributes to care quality and efficiency [ 1 , 2 ]. Among others, it is highly relevant for the care of patients with chronic conditions or complex needs, who frequently transit across different levels of care over time [ 3 , 4 ]. It has been addressed in the last decades by a range of policies and organisational strategies to promote care coordination [ 5 , 6 , 7 ], which underwent a rapid transformation during the pandemic [ 8 , 9 ].
Clinical coordination is here defined [ 10 ] as the harmonious connection of the different health services needed to provide care to a patient throughout the care continuum to achieve a common objective without conflicts and it is analysed based on a comprehensive theoretical framework [ 11 , 12 ]. Two types are distinguished [ 12 ]: (a) clinical information coordination, that refers to the transfer and use of the patient clinical information between providers and (b) clinical management coordination, which involves healthcare provision in a sequential and complementary way and encompasses three dimensions: consistency of care, adequate patient follow-up and accessibility between levels. Clinical coordination is influenced, among others, by organisational factors, such as institutional support, the existing cross-level coordination mechanisms, time available to coordinate and integration of providers’ management [ 13 ] and interactional factors, such as knowledge between doctors or attitudinal factors, job satisfaction [ 13 ].
During the COVID-19 pandemic, several organisational changes were introduced in the health services, to reduce the risk of contagion while maintaining an appropriate response to the population healthcare needs [ 8 , 9 , 14 ], the effects of which on clinical coordination and its related factors is unknown. On the one hand, there was an acceleration in the introduction of information and communication technologies (ICT) based-coordination mechanisms [ 8 , 15 , 16 ], such as shared electronic medical records (EMR) or electronic consultations between PC and secondary care (SC) [ 8 , 16 ], which should have increased cross-level clinical information coordination by facilitating transfer of information between levels [ 2 ] and clinical management coordination by improving access to SC and adequacy of referrals [ 17 ]. On the other hand, the cancellation of non-urgent treatments, tests, or consultations [ 8 ], especially during the first waves of the pandemic, and the introduction of telephone triage [ 8 ] and the rapid adoption of telemedicine [ 9 , 18 ] opened new avenues of access to services that increased professionals workload, especially in PC [ 19 ], decreasing the time available to coordinate with the other level [ 8 ].
Despite its relevance, international evidence on cross-level clinical coordination during the pandemic is scarce. No methodological solid studies have been identified and the few reports mostly based on clinical records review of specific health services focused on evaluating one dimension of clinical coordination, accessibility between levels, reporting a global backlog in access especially to SC [ 20 , 21 ]. The analysis of changes in factors influencing coordination is even more limited, and mostly explored by surveys to SC doctors that analysed job satisfaction during the pandemic [ 22 , 23 ].
The Catalan NHS is part of the Spanish NHS, which is funded by taxes, of universal access and decentralised to the regions [ 24 ]. The provision of healthcare is organised into two care levels: PC, which acts as the gatekeeper and coordinator of the patient care throughout the care continuum, and SC that acts as a consultant to PC and is responsible for the management of more complex procedures [ 24 ]. in the Catalan NHS, patient care is the responsibility of a variety of providers: a large public entity, the Catalan Health Institute, and several public consortia, municipal foundations, and some private foundations (mostly non-profit but also some for-profit), which make up the Integrated Healthcare System for Public Use [ 25 ]. This diversity has originated differences in the type of management of PC and SC providers across the different healthcare areas (1) integrated: PC and SC providers are mostly managed by the same entity; (2) partially integrated: an entity manages SC and some PC centres, while the rest are managed by other entities, and (3) non-integrated: where PC and SC are managed by different entities [ 26 , 27 ]. This complexity makes cross-level coordination even more relevant. Before the pandemic, the Catalan NHS had implemented several strategies, such as promoting integrated management or the introduction of a variety of coordination mechanisms, such as case managers, liaison nurses or shared protocols between levels, including ICT-based mechanisms, such as shared EMRs and electronic consultations between professionals [ 28 ], with great differences in implementation between areas and services [ 29 ]. Analysis on the changes during the pandemic in Spain or Catalonia are limited to few studies on accessibility of specific SC services that reported an increase in waiting times [ 30 , 31 ] and a survey to PC doctors showing a low perception of clinical coordination between levels [ 32 ]. Regarding influencing factors, a study showed an increase in the use of electronic consultations [ 31 ] and a low satisfaction with the job was reported by a survey to SC doctors in training [ 33 ].
This study allowed us to explore whether there were any changes in cross-level clinical coordination and influencing factors in the Catalan health system during the pandemic and identify elements to guide strategies for improving it.
The aim of this study, which forms part of a wider research [ 34 ], is to analyse the changes in the experience, perception of cross-level clinical coordination of primary care (PC) and secondary care (SC) doctors and related factors in the Catalan health system between 2017 and 2022.
Study design and areas of study
A comparative analysis was conducted of two cross-sectional studies based on the online surveys by means of the self-administration of the COORDENA-CAT (2017) and COORDENA-TICs (2022) questionnaires by primary (PC) and secondary care (SC) doctors of the Catalan National Health System. In both years, the areas of study were defined based on the primary healthcare areas (PCC) and their referral hospitals (acute, and in 2017 also long-term care).
Study population and sample
The study population consisted of PC and SC doctors that had been working for at least one year in the organisation, and whose daily practice involved direct contact with patients, and with doctors of the other care level. Specialists in pathology, immunology, neurophysiology, radiology, pharmacy and clinical analysis and preventive medicine were excluded. In both surveys, the selection of the sample took place in two stages. In the first, 41 healthcare areas and its organisations belonging to the Catalan public health system were invited to participate (in 2022, starting by those that had already participated in 2017). In the second, those organisations that agreed to participate, sent an invitation with the questionnaire to all doctors who met the inclusion criteria. The final sample in 2017 was 3,308 doctors of 15,813 invited to participated (21% participation rate) and in 2022, a total of 2,277 doctors of 12,987 invited (17.5% participation rate). Of the 41 healthcare areas invited, in 2017, 32 areas participated both with primary care centres and hospitals, while in 2022, 22 areas did so.
Questionnaire
In 2017, the COORDENA questionnaire, which had been developed following the theoretical framework underlying this study [ 35 ] was adapted, pre-tested, piloted, and validated for the Catalan context [ 36 ]. It consists of three main sections: the first measures doctors’ experience of cross-level clinical information and clinical management coordination and perception of coordination within the healthcare area, by means of 12 items (described in detail in the variables of analysis section) and using a Likert scale and two open-ended questions on their reasons for that perception and suggestions for improvement. The second section measures the availability and use of cross-level clinical coordination mechanisms (shared electronic medical records (EMR), electronic consultations, telephone consultations, email consultations, joint clinical case conference, liaison nurses, shared protocols, and guidelines); and the third, individual, organisational and interactional factors that influence clinical coordination. In 2022, the questionnaire was slightly modified and renamed as COORDENA-TICs [ 34 ]. This new version keeps all main sections and all items of doctors’ experience of cross-level clinical information and clinical management coordination, perception of coordination and of factors related to clinical coordination. The adaptation relies in the coordination mechanisms section, that focuses on ICT-based coordination mechanisms but maintaining the items. Additional items related to the pandemic and some characteristics of use of some mechanisms were included but were not analysed in this study [Additional file 1 ].
Data collection
Data collection for the first survey took place between October and December in 2017 and for the second, between May and June of 2022 and October 2022 to April 2023. In both surveys, all PC and SC doctors who met the inclusion criteria of the organisations that agreed to participate, were invited to answer the questionnaire. To promote doctors’ participation, the involved organisations conducted informative sessions and displayed posters and posts in their institutional intranets. The invitation was sent to their corporate e-mail address, and included a link randomly generated that provided anonymous access to the questionnaire. The participants had the possibility of closing the incomplete questionnaire and retaking it on another occasion, and as many times as they wished, as long as it had not been sent.
Variables of analysis
The outcome variables were (a) experience of cross-level coordination of clinical information (information transfer and use; 3 items) and of clinical management (consistency of care, adequate follow-up, and accessibility; 11 items); (b) general perception of cross-level coordination in the area (1 item); (c) organisational, interactional, and attitudinal related factors (8 items); (d) use of ICT-based coordination mechanisms (shared EMR of the region (HC3/HES) and of the organisation and, electronic consultations through EMR, telephone consultations, email consultations and joint clinical session through videoconference (in 2022) (12 items). The explanatory variables were stratification variables : year and level of care and, adjustment variables : (a) sociodemographic: sex, type of speciality (clinical and surgical/clinical-surgical), (b) employment characteristics: years working as a doctor (c) type of hospital (local/regional, high-resolution, high-technology); and type of area according to the management of PC/SC (integrated, partially integrated, non-integrated).
A bivariate descriptive analysis stratified by level of care (primary and secondary care) and year was conducted to determine the distribution of the outcome and explanatory variables. To identify differences between years in total and within the subgroups, the Chi-square test was used. To analyse the changes in the degree of clinical coordination and related factors including use of ICT-based coordination mechanisms between the two years in the total sample and within the levels of care, Poisson regression models with robust variance were estimated, obtaining prevalence ratios (PR) and their 95% confidence intervals (CI 95%), adjusting for the explanatory variables: level of care, sex, years working as a doctor, type of specialty, and type of hospital, in the case of the aggregated analysis of the sample. And sex, years working as a doctor, type of specialty, and type of hospital for the subgroup analysis. Type of area according to the management of PC/SC was used to control for a possible cluster effect. Participants who answered don’t know/no answer were excluded. Bayesian and Akaike reporting criteria were used to assess the fitness of the models.
Missing values were low for the outcome variables related to the experience and perception of clinical coordination (0.66–7.26%) and those related to factors and use of coordination mechanisms varied from 2.23 to 17.35% and were at random [see Additional file 2 ]. Percentage of missing values for explanatory variables varied from 0 to 19.46% and were at random [see Additional file 2 ]. A full case analysis to manage missing values was adopted. To make the results more robust, sensitivity analyses were performed to evaluate two alternative scenarios (1) analysis of the data after doing multiple imputation of those variables with a percentage of missing values higher than 10% [see Additional file 2 ] and (2) analysis of the data including the participants who answered do not know/no answer to the questions [see Additional file 3 ]. In both cases, there were not significant differences with the results presented in this article. Finally, a content analysis was performed for the open-ended questions on reasons for the general perception of cross-level clinical coordination in the healthcare area and suggestions for improvement in 2022. The answers were coded and classified into categories. Frequencies were calculated and presented stratified by level of care. Statistical analyses were conducted using Stata v.15.
Characteristics of the sample
The sample composition was similar in both study years, with some differences. In 2022, most doctors still were women, but the proportion slightly decreased in PC (68.51% in 2017 to 66.50%) and increased in SC (51.76–53.62%) and in both levels most doctors still were between 41 and 55 years of age. Most doctors in both levels had clinical specialities, but the proportion of doctors with surgical (9.23% in 2017 to 14.85%) and medical/surgical (12.37% in 2017 to 23.31%) specialities considerably increased in SC and dropped almost to zero in PC [Table 1 ]. Regarding employment characteristics, one third of SC doctors still had 11–20 years’ work experience and 6 to 15 years working in the organisation (30.09% and 31.34% respectively), while in the case of PC, there was an increase of the doctors who had 21 to 30 years’ work experience (30.67% in 2017 to 38.79%) and 16 to 25 years working in the organisation (33.58% in 2017 to 37.22%). The proportion of doctors with a permanent contract increased in SC (88.10% in 2017 to 92.96%) and decreased in PC (96.31% in 2017 to 93.57%) and in both levels increased those with a full-time contract (PC: 92.71% in 2017 to 96.40%; SC: 91.44% in 2017 to 94.25%). Finally, regarding the type of area, the highest proportion of doctors worked in an area where the same entity manages SC and the majority of PC (44,04% in 2017 and 46,60% in 2022) and this proportion increased in SC (45.22% in 2017 to 50.45%). In terms of the type of hospital, the proportion of doctors working on an area with a high-technology hospital almost doubled (19.38 in 2017 to 38.21%) [Table 1 ].
Changes in doctor’s experience and perception of cross-level clinical coordination
Compared with 2017, the degree of cross-level coordination of clinical information (transfer and use) experienced by doctors was still high in 2022, with a slight increase of those reporting that the information they share is needed for the patient clinical management (PR:1.07, CI 95% 1.03–1.10), which was higher among PC doctors (PR:1.08, CI 95% 1.03–1.12) [Table 2 ].
Regarding cross-level coordination of clinical management, when compared with 2017, there were improvements in the relative high levels of experience but also setbacks in 2022. Regarding consistency of care, there was an increase in the relatively high proportion of doctors who reported agreeing with the treatments prescribed at the other care level (PR:1.02, CI95% 1.01–1.04), which was higher in PC doctors (PR:1.09, CI95% 1.06–1.12). However, there was a worsening in the already very low proportion of doctors who reported that joint patient management plans were established when needed (PR:0.90, CI95% 0.83–0.97) with no differences between levels, and an increase in the repetition of tests (PR:1.19, CI95% 1.06–1.32) [Table 2 ].
Concerning adequate follow-up between levels, when compared with 2017, the high proportion of doctors who considered that patients were adequately referred to SC decreased, and this decrease was higher in SC doctors (PR:0.96, CI95% 0.92–0.99). Likewise, the relatively high proportion of PC doctors who reported that SC doctors send patients to PC when appropriate decreased (PR:0.94, CI95% 0.91–0.97). Although there is still room for improvement, the proportion of PC doctors who reported receiving follow-up recommendations from SC doctors improved (PR:1.16, CI95% 1.09–1.24) and the proportion of doctors of both levels that reported that PC doctors consult with SC doctors doubts on the patient follow-up also increased (PR:1.10, CI95% 1.05–1.15) and this increase was higher among PC doctors [Table 2 ].
Regarding accessibility between levels, there was an increase in the already high proportion of doctors at both levels who reported long waiting times for patients to be seen after being returned to PC (PR: 1.52, CI95% 1.26–1.83), which was higher for SC doctors [Table 2 ].
Finally, the already low perception of cross-level clinical coordination in the healthcare are in 2017 has worsened by 2022 (PR: 0.78, CI95% 0.66–0.93) and more so among SC doctors (PR: 0.78, CI95% 0.69–0.88) [Table 2 ]. Reasons for considering the coordination to be low continued to be the limited direct communication between professionals and the insufficient availability of coordination mechanisms that promote cross-level communication [Fig. 1 ]. In the same line, main suggestions for improvement of cross-level clinical coordination included implementation of joint clinical case conferences and other mechanisms for direct communication between levels, as well as improving the existing coordination mechanisms [Fig. 2 ].

Reasons for a low perception of clinical coordination within the area, total and by level of care. Year 2022

Suggestions for improving coordination, total and by level of care. Year 2022
Changes in factors influencing cross-level clinical coordination, including use of ICT-based coordination mechanisms
Compared with 2017, there was a worsening of some organisational factors that influence cross-level clinical coordination, with an improvement in use of some ICT-based coordination mechanisms in 2022. On the one hand, there was a decrease in the already relatively low proportion of doctors reporting that their organisation’s management facilitated cross-level clinical coordination (PR: 0.78, CI95% 0.75–0.81) or set objectives aimed at cross-level clinical coordination (PR: 0.82, CI95% 0.78–0.87) and this decrease was higher among SC doctors [Table 3 ]. The proportion of those reporting to have enough time to dedicate to coordination, which was already low in 2017, decrease even more in 2022, especially among SC doctors (PR: 0.70, CI95% 0.61–0.81) [Table 3 ].
On the other hand, in 2022 there was an increase, among doctors from both levels of care who had access to [Additional file 4 ] and frequent use of some ICT-based coordination mechanisms such as, the shared EMR of the region (HC3/HES) (PR:1.21, CI95% 1.15–1.27) and the shared EMR of the organisations (PR:1.07, CI95% 1.04–1.11), that was already relatively high. This increase in use for both EMRs was higher among SC doctors, although they continue to be more used by PC doctors. There was also an increase in the relatively low proportion of doctors using electronic consultations between levels through EMR, especially by PC doctors (PR:1.48, CI95% 1.29–1.70) [Table 3 ]. Nonetheless, difficulties in the use of the mechanisms such as contradictory or disorganised information, technical problems, or lack of relevant information were reported [Additional file 5 ]. In addition, participation in joint clinical case conferences (PR: 0.89, CI95% 0.81–0.98) and use of email consultations (PR:0.66 CI95% 0.50–0.88) decreased, especially among PC doctors [Table 3 ].
As for interactional factors related to cross-level clinical coordination, when compared with 2017, the already low proportion of doctors that reported knowing doctors from the other level decreased (PR:0.56 CI95%. 0.43–0.72), especially among PC doctors. While factors such as trusting in the clinical skills of the other level’s doctors and perceiving that their own practice influences the other level’ remained high, with no differences between years or levels. Finally, doctors’ relatively high satisfaction with their job in their organisations fell significantly at both levels of care (PR: 0.91, CI95% 0.89–0.93) [Table 3 ].
Improving cross-level clinical coordination is essential for healthcare systems based on PC, given the increasingly complex health needs of the patients, which often require care by multiple professionals at different levels of care [ 3 , 4 ]. To address this challenge in recent years European healthcare systems have promoted the implementation of ICT-based coordination mechanisms as tools to improve communication and collaboration between professionals, as well as accessibility, quality, and efficiency [ 37 ]. Moreover, the disruption generated by the COVID-19 pandemic to the health services accelerated the introduction of those mechanisms, among other measures, but their impact on clinical coordination and quality of care is unknown and needs to be analysed to guide future strategies and to contribute to increase health systems resilience. This is the first study that comprehensively analyse changes in the experience and perception of clinical coordination of PC and SC doctors, and related factors, in a NHS following the pandemic, allowing the identification of areas for improvement.
Results show, with some differences between levels, that in 2022 the experience of cross-level coordination of clinical information remained relatively high, with slight improvement, while the experience of coordination of clinical management showed both improvements and setbacks related to cross-level care consistency and patient follow-up. Cross-level accessibility continued to be low and, particularly access to PC has worsened. Likewise, the already low perception of clinical coordination in the healthcare area worsened. There were also setbacks in the organisational factors related to coordination, although there was an improvement in the use of some ICT-based coordination mechanisms. In addition, interactional and attitudinal factors worsened.
Changes in the experience of clinical coordination highlights some resilience but also the need for improvement measures
Despite the relatively high experience of coordination of cross-level clinical information that remained in 2022, there was a worsening of some aspects related to consistency of care, such as tests repetition and contraindications and/or duplications of prescribed treatments, which should have improved with the increased use of the ICT-based coordination mechanisms (EMR, electronic consultations). This is probably related, on the one hand, to the difficulties reported such as, technical problems or outdated or contradictory information [ 38 ] and on the other hand, to the uneven implementation throughout the healthcare areas [ 39 , 40 ] due to the diversity of service provision that characterises the Catalan NHS [ 52 , 53 , 54 ], pointing out the difficulties of implementing shared ICT-based coordination mechanisms and the efforts to overcome them [ 15 , 25 , 28 ]. Therefore, it is necessary for the health authority to address the problems related to the interoperability and uneven implementation of EMRs and electronic consultations [ 41 , 42 ], promoting, in collaboration with the different stakeholders, the implementation of a single electronic health record throughout the territory, on which the rest of the ICT-based coordination mechanisms are based [ 43 , 44 ].
Regarding clinical management coordination, there was an improvement in the agreement on prescribed treatments, consultation of doubts by PC and recommendations made by SC that could be related to the increase in the use of electronic consultations through the EMR, whose main use is to request the clinical opinion of colleagues in their area of expertise [ 11 , 17 ]. However, it seems to be insufficient to improve the limited joint definition of individualized treatments plans, which fell even more in 2022. This could be explained by that shared management of patients with complex needs requires other types of direct synchronous feedback mechanisms (e.g., telephone consultations, joint clinical case conferences) [ 11 , 43 , 44 ]. The results of the study show precisely that the low mutual knowledge reported by doctors before the pandemic has been intensified, among others, because of the backlog in the use of mechanisms that allow direct contact such as joint clinical case conferences and the high staff turnover that healthcare organisations have faced during the pandemic [ 45 ], making interaction between professionals even more difficult.
The COVID-19 added pressure to healthcare professionals [ 8 , 19 ] by increasing work overload with subsequent mental stress and exhaustion, especially in PC [ 46 , 47 ], and may have contributed to the increase of inadequate referrals reported by PC and SC doctors. On the one hand, some studies have shown that it may be more difficult for mentally stressed and exhausted doctors to perform an adequate anamnesis [ 48 , 49 ] and thus make proper referrals and, on the other, the increased use of ICT-based mechanisms may have exacerbated the stress [ 50 , 51 ] and increased the unnecessary referrals to SC to release work overload [ 52 ]. Moreover, as some of the PC doctors reported that SC doctors refused referrals without explanation, the lack of proper feedback could lead to repeated unnecessary referrals. So, further research is needed to analyse more in-depth the factors related with this worsening, as well as, to promote strategies to improve the working environment of professionals, since it might have a negative impact on coordination and quality of care.
Finally, the results show an important decrease in the already limited accessibility between levels before the pandemic, with long waiting times to SC, and, particularly to PC. These results are in line with the available evidence [ 20 , 21 , 30 , 31 ] that analyse the consequences of the measures introduced during the pandemic (elective procedures postponed, resources redirected to COVID-19 care, shift to telemedicine, etc.) [ 8 , 20 , 37 , 53 ], that affected the functioning of health services already under pressure (and underfunded) due to the austerity measures introduced during the last financial crisis [ 16 ]. These results call into question the effectiveness of measures that were put in place to improve accessibility during the pandemic, such as the use of electronic consultations between levels [ 16 ]. In this regard, some studies have linked their use to increased barriers of access to SC, as SC doctors could refuse face-to-face referrals until additional tests were performed, among others [ 54 ]. It is also necessary to strengthen access to PC, among others, by promoting reorganisation plans in PC that includes mixed face-to-face/telematic consultations and optimisation of resources, so that it can properly act as the gatekeeper to the NHS and coordinator of patients care throughout the healthcare process [ 8 ].
Reduction in the poor perception of cross-level clinical coordination may be related to setbacks in organisational, interactional, and attitudinal factors during and after the pandemic
Despite maintenance or improvement in some aspects of the experience of clinical coordination between levels, there was a significant worsening in the perception of coordination in the healthcare area, already low before the pandemic, especially among SC doctors. This is congruent with a survey carried out with PC doctors of Catalonia during the first waves of the pandemic that showed a perception of lack of coordination, especially with emergency rooms and hospital outpatient care [ 32 ]. The results of the analysis of changes in factors related to coordination show that this drop may be related to: (1) the decrease in the use of synchronous coordination mechanisms such as joint clinical case conferences that facilitate direct communication, collaboration, and mutual knowledge [ 55 ]; (2) the decrease in institutional support to provide the appropriate conditions for coordination (time, common objectives, etc.); (3) the decrease in job satisfaction, also described in the literature [ 32 , 56 ], and in addition to the above-mentioned factors, to the general worsening of working conditions and the burnout to which they are subjected [ 56 , 57 ], especially in primary care [ 32 ]. The worsening of all these factors, which would have been exacerbated during the first waves of the pandemic, does not seem to have been reversed in the subsequent phases. Therefore, it is necessary to further analyse the causes of the high job dissatisfaction of professionals and organisational factors such as institutional support, to promote the implementation of strategies for their improvement.
Improving doctors’ mutual knowledge and existing coordination mechanisms: strategies proposed by doctors to improve cross-level coordination
Results on doctors’ suggestions to improve clinical coordination between levels referred to improving organisational and interactional factors and are consistent with previous results [ 58 ], highlighting the way forward and the relevance of involving professionals in the selection and design of interventions [ 59 ]. First, they suggested the implementation of mechanisms that promote direct communication and knowledge between professionals, essential factors to improve the experience and perception of coordination [ 60 , 61 ]. Although ICT-based coordination mechanisms (e.g., shared EMR or electronic consultations) have been introduced to address this issue [ 28 ], due to their potential for improving transfer of clinical information and communication between professionals [ 17 , 38 ], they need to be used in combination with others that allow verbal communication, feedback and standardisation of processes [ 40 , 55 , 58 , 62 ] -specifically joint clinical case conferences, direct synchronous communication channels (telephone) between PC and SC and shared protocols-, even though they are more time consuming, they allow to establish common clear pathways of diagnosis and treatment and collaboration [ 40 , 55 ]. Hence, the importance of facilitating an organisational environment that allows their proper use: time and an increase in needed resources [ 63 ].
Second, they suggested the improvement of the existing coordination mechanisms, in keeping with the evidence that difficulties -especially those affecting interoperability and safety- can discourage their use and limit the impact on clinical coordination [ 38 , 42 , 51 ]. Interventions for improving clinical coordination are often introduced but are not designed or evaluated in a participatory way [ 64 ], although the involvement of professionals in the process can be relevant to correct deficiencies or difficulties that may arise and generates greater acceptance, increasing its sustainability over time [ 65 ]. In short, results show the need for development of multicomponent strategies that include the participation of professionals in the identification of difficulties and design of mechanisms, since their involvement is key to adapt the strategies to the conditions and needs of each context to ensure that they can be properly implemented [ 59 ].
One of the potential limitations of this study is that there may have been a selection bias due to the self-administered nature of the questionnaire and the non-probabilistic sampling of the areas. Nevertheless, the characteristics of the sample were similar to the universe of doctors in the Catalan NHS [ 66 , 67 , 68 ] and the diversity of the health areas of the Catalan Health System was represented. Finally, a drop in participation in 2022, which may have been influenced by the critical time in which the survey was conducted, the beginning of the recovery after the increase in infections by the omicron variant of COVID-19 [ 69 ]. Nevertheless, the participation rate was within the expected range for an online survey [ 70 ].
The COVID-19 pandemic was a challenging milestone that put a great pressure on health systems. It led to the rapid adoption of strategies to ensure healthcare to the population such as ICT-based coordination mechanisms. However, its impact on clinical coordination is unknow. This study analysed the changes in the different dimensions of cross-level clinical coordination and related factors that occurred in the Catalan NHS after the pandemic. Its results help to identify areas of improvement and make recommendations that are also useful for others NHS.
Even though there was an increased use of coordination mechanisms such as shared EMRs or electronic consultations and an improvement in some elements of coordination of clinical information and of clinical management probably related to a greater use of these mechanisms, other aspects of coordination such as the adequacy of referrals and accessibility between care levels have worsened, contrary to expected. Therefore, further evaluation of the impact of ICT-based coordination mechanisms on care coordination, and the barriers and facilitators associated to its use, is needed. Likewise, particular attention must be paid to other issues that worsened and are associated to the low perception of general coordination seen such as institutional support for coordination, knowledge between doctors, and job satisfaction, as well as to the contextual elements that give rise to them and that have intensified following the pandemic, such as increased waiting lists, work overload, high staff turnover and worse working conditions.
In consequence, decision makers and managers would have to prioritise participatory strategies that facilitate direct communication and knowledge between professionals and to foster an organisational climate that facilitates its implementation and sustainability, as well as to address the difficulties detected in the existing ones. It is also necessary to encourage support and protection policies for healthcare professionals and services that improve the working environment, promote cross-level clinical coordination, and guarantee quality and efficient care for more resilient NHS.
Data availability
No datasets were generated or analysed during the current study.
Abbreviations
National Health System
Primary Care
Secondary Care
Electronic medical record
Ovretveit J. Does clinical coordination improve quality and save money - A summary review of the evidence. The health foundation [Internet]. 2011;2(June):1–30. http://www.ncbi.nlm.nih.gov/pubmed/21325659
Motulsky A, Sicotte C, MP M, Schuster T, Girard N, Buckeridge D et al. Using Health Information Exchange: Usage and Perceived Usefulness in Primary Care. Stud Health Technol Inform [Internet]. 2019;264:709–13. https://pubmed.ncbi.nlm.nih.gov/31438016/
Sampson R, Cooper J, Barbour R, Polson R, Wilson P. Patients’ perspectives on the medical primary–secondary care interface: systematic review and synthesis of qualitative research. BMJ Open. 2015;5(10):e008708.
PubMed PubMed Central Google Scholar
Bywood P, Jackson-Bowers E, Muecke S. Initiatives to integrate primary and acute health care, including ambulatory care services. Adelaide: Primary Health Care Research & Information Service; 2011.
Google Scholar
Simpson K, Nham W, Thariath J, Schafer H, Greenwood-Eriksen M, Fetters MD et al. How health systems facilitate patient-centered care and care coordination: a case series analysis to identify best practices. BMC Health Serv Res [Internet]. 2022;22(1):1448. https://bmchealthservres.biomedcentral.com/articles/ https://doi.org/10.1186/s12913-022-08623-w
Graetz I, Reed M, Shortell S, Rundall T, Bellows J, Hsu J et al. The next step towards making use meaningful: electronic information exchange and care coordination across clinicians and delivery sites. Med Care [Internet]. 2014;52(12):1037–41. https://pubmed.ncbi.nlm.nih.gov/25304020/
Vimalananda VG, Orlander JD, Afable MK, Fincke BG, Solch AK, Rinne ST et al. Electronic consultations (E-consults) and their outcomes: a systematic review. Journal of the American Medical Informatics Association [Internet]. 2020;27(3):471–9. https://academic.oup.com/jamia/article/27/3/471/5588944
Satué de Velasco E, Gayol Fernández M, Eyaralar Riera MT, Magallón Botaya R, Abal Ferrer F. Impact of the pandemic on primary care. SESPAS Report 2022. Gac Sanit. 2022;36:S30–5.
Mohammed HT, Hyseni L, Bui V, Gerritsen B, Fuller K, Sung J et al. Exploring the use and challenges of implementing virtual visits during COVID-19 in primary care and lessons for sustained use. Prazeres F, editor. PLoS One [Internet]. 2021;16(6):e0253665. https://doi.org/10.1371/journal.pone.0253665
Longest B, Young G. Coordination and communication. In: Shortell S, Kaluzny A, editors. Healthcare Management: Organization Design and Behavior. 4th ed. New York: Delmar; 2000. pp. 210–43.
Terraza R, Vargas I, Vázquez ML. La coordinación entre niveles asistenciales: una sistematización de sus instrumentos y medidas. Gac Sanit. 2006;20(6):485–95.
Reid R, Haggerty JM. Defusing the Confusion: Concepts and Measures of Continuity of Healthcare. [Internet]. Ottawa, Ontario; 2002. https://www.researchgate.net/publication/245856177_Defusing_the_Confusion_Concepts_and_Measures_of_Continuity_of_Health_Care
Vázquez ML, Vargas I, Garcia-Subirats I, Unger JP, De Paepe P, Mogollón-Pérez AS et al. Doctors’ experience of coordination across care levels and associated factors. A cross-sectional study in public healthcare networks of six Latin American countries. Soc Sci Med [Internet]. 2017;182:10–9. https://linkinghub.elsevier.com/retrieve/pii/S0277953617302241
Pérez A. Retos, logros y dificultades del médico de familia ante la pandemia por COVID-19 en Andalucía. Actual Med [Internet]. 2021;106(814):Supl2: 109–117. https://actualidadmedica.es/articulo-suplementos/supl814-2_re15/
Servei Català de la Salut. Generalitat de Catalunya. Mapa estratègic CatSalut 2022–2024. Reptes i full de ruta. 2022.
Fahy N, Williams GA, Habicht T et al. Use of digital health tools in Europe: Before, during and after COVID-19 [Internet]. Copenhague; 2021 [cited 2022 Feb 10]. https://www.ncbi.nlm.nih.gov/books/NBK576970/pdf/Bookshelf_NBK576970.pdf
Vimalananda VG, Gupte G, Seraj SM, Orlander J, Berlowitz D, Fincke BG, et al. Electronic consultations (e-consults) to improve access to specialty care: a systematic review and narrative synthesis. J Telemed Telecare. 2015;21(6):323–30.
Jiménez Carrillo M, Martín Roncero U, Aldasoro Unamuno E, Morteruel Arizcuren M, Baza Bueno M. Percepciones y experiencias de la población ante la transformación de la modalidad de las consultas en atención primaria durante la pandemia. Aten Primaria. 2022;54(4):102263.
Ares-Blanco S, Astier-Peña MP, Gómez-Bravo R, Fernández-García M, Bueno-Ortiz JM. The role of primary care during COVID-19 pandemic: a European overview. Aten Primaria. 2021;53(8).
van Ginneken E, Reed S, Siciliani L, Eriksen A, Schlepper L, Tille F et al. Addressing backlogs and managing waiting lists during and beyond the COVID-19 pandemic. 2022.
NHS Staff Survey Co-ordination Centre. NHS Staff Survey National Results. London; 2021.
House S, Crandell J, Stucky C, Kitzmiller R, Jones C, Gittell JH. Relational Coordination as a Predictor of Job Satisfaction and Intent to Stay Among Nurses and Physicians in the Military Health System. Mil Med [Internet]. 2023;188(1–2):e316–25. https://academic.oup.com/milmed/article/188/1-2/e316/6432365
Capone V, Borrelli R, Marino L, Schettino G. Mental Well-Being and Job Satisfaction of Hospital Physicians during COVID-19: Relationships with Efficacy Beliefs, Organizational Support, and Organizational Non-Technical Skills. Int J Environ Res Public Health [Internet]. 2022;19(6):3734. https://www.mdpi.com/1660-4601/19/6/3734
Bernal-Delgado E, Garcia-Armesto S, Oliva J, Sanchez Martinez FI, Repullo JR, Pena-Longobardo LM et al. Spain: Health System Review. Health Syst Transit [Internet]. 2018;20(2):1–179. http://www.ncbi.nlm.nih.gov/pubmed/30277216
Direcció General de Planifcació en Salut. Pla de salut de Catalunya 2021–2025 [Internet]. Barcelona, Spain. 2021. https://hdl.handle.net/11351/7948
Esteve-Matalí L, Vargas I, Cots F, Ramon I, Sánchez E, Escosa A, et al. Does the integration of health services management improve clinical coordination? Experience in Catalonia. Gac Sanit. 2022;36(4):324–32.
PubMed Google Scholar
Vargas I, Vázquez ML, Henao D, Calpe JF. De la competència a la col·laboració. Experiència en la integració assistencial a Catalunya. Fulls econòmics del sistema sanitari [Internet]. 2009;38:27. https://dialnet.unirioja.es/servlet/articulo?codigo=3492040
Generalitat de Catalunya. Departament de salut. The Catalan Information Systems Master Plan: Building a digital health strategy for Catalonia together [Internet]. 2017. https://salutweb.gencat.cat/web/.content/_ambits-actuacio/Linies-dactuacio/tic/pdsis/pdsis-en.pdf
Vazquez ML, Amigo F, Esteve-Matalí L, Vargas I. La coordinación clínica entre niveles de atención: Resultados comparativos entre áreas del sistema sanitario en Cataluña [Internet]. Barcelona, Spain; 2021. http://www.consorci.org/media/upload/arxius/coneixement/COORDENA.CAT/cast Informe general Coordena CAT_final2.pdf.
García-Rojo E, Manfredi C, Santos-Pérez-de-la-Blanca R, Tejido-Sánchez, García-Gómez B, Aliaga-Benítez M, et al. Impact of COVID-19 outbreak on urology surgical waiting lists and waiting lists prioritization strategies in the Post-COVID-19 era. Actas Urol Esp. 2021;45(3):207–14.
Pavón I, Rosado Sierra J, Salguero Ropero A, Viedma Torres V, Guijarro de Armas G, Cuesta Rodríguez-Torices M et al. [E-consultation as a tool for the relationship between Primary Care and Endocrinology. Impact of COVID-19 epidemic in its use]. J Healthc Qual Res [Internet]. 2022;37(3):155–61. https://pubmed.ncbi.nlm.nih.gov/34866028/
Societat Catalana de Medicina Familiar i Comunitària. Atenció Primària en l’era post-COVID: revolució per a la transformació. Barcelona; 2021.
Muñoz-Cobo Orosa B, Pérez García M, Rodríguez Ledott M, Varela Serrano C, Sanz Valero J. Satisfacción laboral y calidad de vida de Los médicos residentes españoles durante la pandemia por la COVID-19. Med Segur Trab (Madr). 2022;67(264):169–90.
Campaz D, Vargas I, Plaja P, Sanclemente M, Paino M, Madrid M et al. A questionnaire to measure the impact of ICT-based coordination mechanisms on clinical coordination. Eur J Public Health [Internet]. 2022;32(Supplement_3). https://academic.oup.com/eurpub/article/doi/ https://doi.org/10.1093/eurpub/ckac130.118/6765902
Vazquez ML, Vargas I, Unger JP, De Paepe P, Mogollon-Perez AS, Samico I, et al. Evaluating the effectiveness of care integration strategies in different healthcare systems in Latin America: the EQUITY-LA II quasi-experimental study protocol. BMJ Open. 2015;5(7):e007037.
Vázquez ML, Vargas I, Romero A, Sánchez E, Ramon I, Plaja P, et al. Adapting the COORDENA questionnaire for measuring clinical coordination across health care levels in the public health system of Catalonia (Spain). Public Health Panorama. 2018;4(4):491–735.
Fahy N, Williams GA, Habicht T, et al. Use of digital health tools in Europe: before, during and after COVID-19. Copenhague; 2021.
Motulsky A, Sicotte C, MP M, Schuster T, Girard N, Buckeridge D, et al. Using Health Information Exchange: usage and Perceived Usefulness in Primary Care. Stud Health Technol Inf. 2019;264:709–13.
Schoen C, Osborn R, Squires D, Doty M, Rasmussen P, Pierson R et al. A Survey Of Primary Care Doctors In Ten Countries Shows Progress In Use Of Health Information Technology, Less In Other Areas. Health Aff [Internet]. 2012;31(12):2805–16. http://www.healthaffairs.org/doi/10.1377/hlthaff.2012.0884
Aller MB, Vargas I, Coderch J, Vázquez ML. Doctors’ opinion on the contribution of coordination mechanisms to improving clinical coordination between primary and outpatient secondary care in the Catalan national health system. BMC Health Serv Res. 2017;17(1):1–11.
Li E, Clarke J, Ashrafian H, Darzi A, Neves AL. The Impact of Electronic Health Record Interoperability on Safety and Quality of Care in High-Income countries: systematic review. J Med Internet Res. 2022;24(9):e38144.
Dutta B, Hwang HG. The adoption of electronic medical record by physicians. Medicine. 2020;99(8):e19290.
Secretaria General de Salud Digital Información e Innovación para el SNS. Estrategia de salud digital: Sistema Nacional de Salud [Internet]. 2021. https://www.sanidad.gob.es/ciudadanos/pdf/Estrategia_de_Salud_Digital_del_SNS.pdf
Miloris K, Papageorgiou K. A Study on Healthcare ICT Systems and their Usefulness During CoVid-19 Focused in the European Environment. Journal of Hospital and Healthcare Administration [Internet]. 2021;5(1). https://www.gavinpublishers.com/article/view/a-study-of-healthcare-ict-systems-and-their-usefulness-during-covid19-focused-in-the-european-environment-1
Randstad Research. Informe de rotación laboral en España 2022. 2022. Available on: https://www.randstadresearch.es/informe-rotacion-2022/
Seda-Gombau G, Montero-Alía JJ, Moreno-Gabriel E, Torán-Monserrat P. Impact of the COVID-19 pandemic on Burnout in Primary Care Physicians in Catalonia. Int J Environ Res Public Health. 2021;18(17):9031.
CAS PubMed PubMed Central Google Scholar
Prasad K, McLoughlin C, Stillman M, Poplau S, Goelz E, Taylor S, et al. Prevalence and correlates of stress and burnout among U.S. healthcare workers during the COVID-19 pandemic: a national cross-sectional survey study. EClinicalMedicine. 2021;35:100879.
Kushnir T, Greenberg D, Madjar N, Hadari I, Yermiahu Y, Bachner YG. Is burnout associated with referral rates among primary care physicians in community clinics? Fam Pract. 2014;31(1):44–50.
Mangory KY, Ali LY, Rø KI, Tyssen R. Effect of burnout among physicians on observed adverse patient outcomes: a literature review. BMC Health Serv Res. 2021;21(1):369.
Bahr TJ, Ginsburg S, Wright JG, Shachak A. Technostress as source of physician burnout: an exploration of the associations between technology usage and physician burnout. Int J Med Inf. 2023;177:105147.
Osman MA, Schick-Makaroff K, Thompson S, Bialy L, Featherstone R, Kurzawa J, et al. Barriers and facilitators for implementation of electronic consultations (eConsult) to enhance access to specialist care: a scoping review. BMJ Glob Health. 2019;4(5):1–16.
Gupte G, Vimalananda V, Simon SR, DeVito K, Clark J et al. Disruptive innovation: implementation of electronic consultations in a veterans affairs health care system. JMIR Med Inf. 2016;4(1):e6.
Pujolar G, Oliver-Anglès A, Vargas I, Vázquez ML. Changes in Access to Health Services during the COVID-19 pandemic: a scoping review. Int J Environ Res Public Health. 2022;19(3):1749.
Lee MS, Ray KN, Mehrotra A, Giboney P, Yee HF, Barnett ML. Primary care practitioners’ perceptions of electronic Consult systems. JAMA Intern Med. 2018;178(6):782.
Henao D, Vázquez ML, Vargas I. Factores que influyen en la coordinación entre niveles asistenciales según la opinión de directivos y profesionales sanitarios. Gac Sanit. 2009;23(4):280–6.
Alrawashdeh HM, Al-Tammemi AB, Alzawahreh MKh, Al-Tamimi A, Elkholy M, Al Sarireh F, et al. Occupational burnout and job satisfaction among physicians in times of COVID-19 crisis: a convergent parallel mixed-method study. BMC Public Health. 2021;21(1):811.
Costello H, Walsh S, Cooper C, Livingston G. A systematic review and meta-analysis of the prevalence and associations of stress and burnout among staff in long-term care facilities for people with dementia. Int Psychogeriatr. 2019;31(08):1203–16.
Esteve-Matalí L, Vargas I, Amigo F, Plaja P, Cots F, Mayer EF, et al. Understanding how to improve the use of clinical coordination mechanisms between primary and secondary care doctors: clues from Catalonia. Int J Environ Res Public Health. 2021;18(6):1–18.
Colquhoun HL, Squires JE, Kolehmainen N, Fraser C, Grimshaw JM. Methods for designing interventions to change healthcare professionals’ behaviour: a systematic review. Implement Sci. 2017;12(1):1–11.
Aller MB, Vargas I, Coderch J, Calero S, Cots F, Abizanda M et al. Doctors’ opinions on clinical coordination between primary and secondary care in the Catalan healthcare system. Gac Sanit. 2019.
Esteve-Matalí L, Vargas I, Sánchez E, Ramon I, Plaja P, Vázquez ML. Do primary and secondary care doctors have a different experience and perception of cross-level clinical coordination? Results of a cross-sectional study in the catalan national health system (Spain). BMC Fam Pract. 2020;21(1).
Collins SA, Bakken S, Vawdrey DK, Coiera E, Currie L. Clinician preferences for verbal communication compared to EHR documentation in the ICU. Appl Clin Inf. 2011;02(02):190–201.
CAS Google Scholar
Mitchell GK, Del Mar CB, Clavarino AM, Jong IC, Kennedy R. General practitioner attitudes to case conferences: how can we increase participation and effectiveness? Medical Journal of Australia. 2002;177(2):95–7.
Tang T, Lim ME, Mansfield E, McLachlan A, Quan SD. Clinician user involvement in the real world: Designing an electronic tool to improve interprofessional communication and collaboration in a hospital setting. Int J Med Inf. 2018;110:90–7.
Loewenson R, Laurell AC, Hogstedt C, D’Ambruoso L, Shroff Z. Participatory action research in health systems: a methods reader. AHPSR, WHO, IDRC Canada, Equinet: TARSC; 2014.
Solsona i Pairó M, Treviño R, Merino M, Ferrer L. Demografia de les Professions Sanitàries a Catalunya: Anàlisi dels Estocs Actuals de Professionals Sanitari. Barcelona, Spain; 2006.
Instituto de estadística de Cataluña. Personal hospitalario. Por categorias, tipos de concierto y tipos de hospital Cataluña. Internet. 2017;2019(cited 2024 Mar 5):Availablefromhttpswwwidescatcatindicadors–idaecn15813.
Instituto nacional de estadística. N o de Médicos por Comunidades, Ciudades autónomas y Provincias de colegiación, edad y sexo. [Internet]. 2022 [cited 2023 Oct 13]. https://www.ine.es/jaxi/Tabla.htm?tpx=59167&L=0
Cunningham CT, Quan H, Hemmelgarn B, Noseworthy T, Beck CA, Dixon E, et al. Exploring physician specialist response rates to web-based surveys. BMC Med Res Methodol. 2015;15(1):32.
Smyth J, Pearson J. Internet survey methods: a review of strengths, weaknesses, and innovations. In: Das M, Este P, Kaczmirek L, editors. Social and behavioral research and the internet advances in applied methods and research strategies. New York: Taylor and Francis Group; 2011. pp. 11–43.
Download references
Acknowledgements
We highly appreciate the contributions to the data collection of the members who, together with the authors of the paper, constitute the Healthcare Integration Evaluation Group (GAIA): Alex Escosa (Institut Català de la Salut), Marta Banqué (Consorci Sanitari de l’Anoia), Rami Qanneta (Gestió i Prestació de Serveis de Salut). We also thank Marcos Azuaga for the online programming of the questionnaires and Palmira Borràs, Verónica Espinel, Aida Oliver, Zahara Lucena (Consorci de Salut i Social de Catalunya) for their support.
This study analyses data that were collected as part of two research projects, “The coordination between levels of care and its relationship with the quality of care in different healthcare environments of the public health system (COORDENA-CAT project, 2017) (PI15/0021)” and “Impact of ICT-based coordination mechanisms on clinical coordination and care quality in the National Health System (COORDENA-TICs project, 2022) (PI20/00290)”, both partially funded by Carlos III Health Institute and the European Regional Development Fund. The funding body did not participate in the study design, data collection, analysis interpretation or in writing the manuscript.
Author information
Authors and affiliations.
Health Policy and Health Services Research Group, Health Policy Research Unit, Consortium for Health Care and Social Services of Catalonia, Barcelona, 08022, Spain
Daniela Campaz-Landazabal, Ingrid Vargas & María Luisa Vázquez
Serveis de Salut Integrats Baix Empordà - Hospital de Palamós. Unitat d’Inf. Assistencial, Palamós, 17230, Spain
Elvira Sánchez
Parc de Salut Mar, Barcelona, 08003, Spain
Francesc Cots
Fundació Salut Empordà, Figueres, 17600, Spain
Badalona Serveis Assistencials, Badalona, 08911, Spain
Joan Manuel Perez-Castejón
Consorci Sanitari de Terrassa, Terrassa, 08227, Spain
Antonio Sánchez-Hidalgo
You can also search for this author in PubMed Google Scholar
Contributions
ML.V and I.V were responsible for the design and supervision of the study. D.C.L analysed and interpreted the data and wrote the first draft of the manuscript. ML.V, I.V, D.C.L, E.S, F.C, P.P, JM.P.C and A.S.H coordinated data collection, participated in its interpretation and were contributors in writing the manuscript. All authors reviewed and approved the final manuscript.
Corresponding author
Correspondence to Ingrid Vargas .
Ethics declarations
Ethics approval and consent to participate.
The COORDENA-CAT study was carried out in accordance with the current legislation and EU and national conventions and declarations on ethics in research, in full conformance with principles of the Declaration of Helsinki (Fortaleza, Brazil, 2013) and was approved by the ethics committee of Parc de Salut Mar and Bellvitge hospital (code: (2016/6726/I) and the COORDENA-TICs study was approved by the ethics committee of Parc Salut Mar (code: 2020/9645), the research ethics committee of the Balearic Islands (code IB 4774/22) and the ethics committee for drug research of the Basque Country (code: PI2021151). All study participants read and gave their authorization by means of the informed consent prior to completing the survey and could withdraw at any time. The researchers did not have access to any of the participants’ personal data and anonymity was guaranteed by assigning a random code to each participant. The processing, communication, and transfer of personal data of all participating subjects complied with the provisions of the regulation (EU) 2016/679 of 27 April on the protection of personal data.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary material 2, supplementary material 3, supplementary material 4, supplementary material 5, rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ .
Reprints and permissions
About this article
Cite this article.
Campaz-Landazabal, D., Vargas, I., Sánchez, E. et al. Has cross-level clinical coordination changed in the context of the pandemic? The case of the Catalan health system. BMC Health Serv Res 24 , 959 (2024). https://doi.org/10.1186/s12913-024-11445-7
Download citation
Received : 04 December 2023
Accepted : 14 August 2024
Published : 21 August 2024
DOI : https://doi.org/10.1186/s12913-024-11445-7
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Clinical coordination
- Care coordination
- Coordination mechanisms
- ICT-based coordination mechanism
- Primary care
- Secondary care
BMC Health Services Research
ISSN: 1472-6963
- General enquiries: [email protected]
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- Published: 20 August 2024
Spatial sampling bias influences our understanding of early hominin evolution in eastern Africa
- W. Andrew Barr ORCID: orcid.org/0000-0001-9763-6440 1 &
- Bernard Wood ORCID: orcid.org/0000-0003-0273-7332 1
Nature Ecology & Evolution ( 2024 ) Cite this article
Metrics details
- Biological anthropology
- Palaeoecology
- Palaeontology
The eastern branch of the Eastern African Rift System (EARS) is the source of a large proportion of the early hominin fossil record, but it covers a tiny fraction (ca. 1%) of the continent. Here we investigate how this mismatch between where fossils are preserved and where hominins probably lived may influence our ability to understand early hominin evolution, using extant mammals as analogues. We show that the eastern branch of the EARS is not an environmentally representative sample of the full species range for nearly all extant rift-dwelling mammals. Likewise, when we investigate published morphometric datasets for extant cercopithecine primates, evidence from the eastern branch alone fails to capture major portions of continental-scale cercopithecine cranial morphospace. We suggest that extant rift-dwelling species should be used as analogues to place confidence intervals on hominin habitat reconstructions. Furthermore, given the north–south orientation of the eastern branch of the EARS, morphoclines that are not aligned along this major north–south axis are likely to be poorly sampled by sites in the eastern branch. There is a pressing need for research on the geography of early hominin morphoclines to estimate how morphologically representative the hominin fossil sample from the eastern branch may be.
This is a preview of subscription content, access via your institution
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
24,99 € / 30 days
cancel any time
Subscribe to this journal
Receive 12 digital issues and online access to articles
111,21 € per year
only 9,27 € per issue
Buy this article
- Purchase on SpringerLink
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
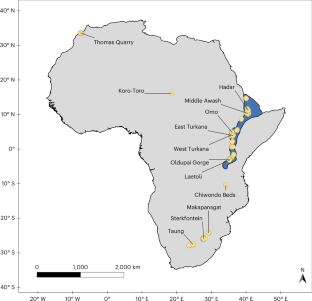
Data availability
Data files necessary for producing the figures and analyses are available on Github at https://github.com/wabarr/outside-rift .
Code availability
Code necessary for producing the figures and analyses is available on Github at https://github.com/wabarr/outside-rift .
Langergraber, K. E. et al. Generation times in wild chimpanzees and gorillas suggest earlier divergence times in great ape and human evolution. Proc. Natl Acad. Sci. USA https://doi.org/10.1073/pnas.1211740109 (2012).
Article PubMed PubMed Central Google Scholar
Kronenberg, Z. N. et al. High-resolution comparative analysis of great ape genomes. Science 360 , eaar6343 (2018).
Diogo, R., Molnar, J. L. & Wood, B. Bonobo anatomy reveals stasis and mosaicism in chimpanzee evolution, and supports bonobos as the most appropriate extant model for the common ancestor of chimpanzees and humans. Sci. Rep. 7 , 608 (2017).
Darwin, C. The Descent of Man and Selection in Relation to Sex (Murray, 1871).
Book Google Scholar
Pickering, R. et al. U–Pb-dated flowstones restrict South African early hominin record to dry climate phases. Nature https://doi.org/10.1038/s41586-018-0711-0 (2018).
Curtis, G. H., Drake, Cerling, T. & Hampel, J. H. Age of KBS Tuff in Koobi Fora Formation, East Rudolf, Kenya. Nature 258 , 395–398 (1975).
Article CAS Google Scholar
Gleadow, A. J. W. Fission track age of the KBS Tuff and associated hominid remains in northern Kenya. Nature 284 , 225–230 (1980).
Campisano, C. J. & Feibel, C. S. Tephrostratigraphy of the Hadar and Busidima Formations at Hadar, Afar Depression, Ethiopia. Geol. Soc. Am. Spec. Pap. 446 , 135–162 (2008).
Google Scholar
Deino, A. L. et al. 40 Ar/ 39 Ar dating, paleomagnetism, and tephrochemistry of Pliocene strata of the hominid-bearing Woranso-Mille area, west-central Afar Rift, Ethiopia. J. Hum. Evol. 58 , 111–126 (2010).
Article PubMed Google Scholar
Cohen, A. et al. The hominin sites and paleolakes drilling project: inferring the environmental context of human evolution from eastern African rift lake deposits. Sci. Drill. 21 , 1–16 (2016).
Article Google Scholar
Leakey, L. S. B. A new fossil skull from Olduvai. Nature 184 , 491–493 (1959).
Leakey, R. E. F. Further evidence of Lower Pleistocene hominids from East Rudolf, North Kenya, 1973. Nature 248 , 653–656 (1974).
Article CAS PubMed Google Scholar
Johanson, D. C. & White, T. D. A systematic assessment of early African hominids. Science 203 , 321–330 (1979).
Walker, A. & Leakey, R. E. F. The Nariokotome Homo erectus Skeleton (Springer, 1993).
Alemseged, Z. et al. A juvenile early hominin skeleton from Dikika, Ethiopia. Nature 443 , 296–301 (2006).
White, T. D. et al. Ardipithecus ramidus and the paleobiology of early hominids. Science 326 , 64–86 (2009).
Haile-Selassie, Y., Melillo, S. M., Vazzana, A., Benazzi, S. & Ryan, T. M. A 3.8-million-year-old hominin cranium from Woranso-Mille, Ethiopia. Nature https://doi.org/10.1038/s41586-019-1513-8 (2019).
Behrensmeyer, A. K., Todd, N. E., Potts, R. & McBrinn, G. E. Late Pliocene faunal turnover in the Turkana Basin, Kenya and Ethiopia. Science 278 , 1589–1594 (1997).
Bobe, R., Behrensmeyer, A. & Chapmam, R. Faunal change, environmental variability and late Pliocene hominin evolution. J. Hum. Evol. 42 , 475–497 (2002).
Levin, N. E., Cerling, T. E., Passey, B. H., Harris, J. M. & Ehleringer, J. R. A stable isotope aridity index for terrestrial environments. Proc. Natl Acad. Sci. USA 103 , 11201–11205 (2006).
Article CAS PubMed PubMed Central Google Scholar
Reed, K. E. Paleoecological patterns at the Hadar hominin site, Afar Regional State, Ethiopia. J. Hum. Evol. 54 , 743–768 (2008).
Potts, R. et al. Increased ecological resource variability during a critical transition in hominin evolution. Sci. Adv. 6 , eabc8975 (2020).
Hill, A. in Hominin Environments in the East African Pliocene: An Assessment of the Faunal Evidence (eds Bobe, R. et al.) xvii–xx (Springer, 2007).
Kidwell, S. M. & Holland, S. M. The quality of the fossil record: implications for evolutionary analyses. Annu. Rev. Ecol. Syst. 33 , 561–588 (2002).
Benson, R. B. J., Butler, R., Close, R. A., Saupe, E. & Rabosky, D. L. Biodiversity across space and time in the fossil record. Curr. Biol. 31 , R1225–R1236 (2021).
Holland, S. M. The non-uniformity of fossil preservation. Philos. Trans. R. Soc. B 371 , 20150130 (2016).
Behrensmeyer, A. K., Kidwell, S. M. & Gastaldo, R. A. Taphonomy and paleobiology. Paleobiology 26 , 103–147 (2000).
Kottek, M., Grieser, J., Beck, C., Rudolf, B. & Rubel, F. World Map of the Köppen–Geiger climate classification updated. Meteorol. Z. 15 , 259–263 (2006).
Nyberg, B. & Howell, J. A. Is the present the key to the past? A global characterization of modern sedimentary basins. Geology 43 , 643–646 (2015).
Hopley, P. J. & Maxwell, S. J. in African Paleoecology and Human Evolution (eds Reynolds, S. C. & Bobe, R.) 15–23 (Cambridge Univ. Press, 2022); https://doi.org/10.1017/9781139696470.003
Maxwell, S. J., Hopley, P. J., Upchurch, P. & Soligo, C. Sporadic sampling, not climatic forcing, drives observed early hominin diversity. Proc. Natl Acad. Sci. USA https://doi.org/10.1073/pnas.1721538115 (2018).
Morley, C. K., Ngenoh, D. K. & Ego, J. K. in Geoscience of Rift Systems—Evolution of East Africa (ed. Morley, C. K.) 1–18 (AAPG Studies in Geology, 1999).
Ebinger, C. Continental break-up: the East African perspective. Astron. Geophys. 46 , 2.16–2.21 (2005).
Frost, S. R., Marcus, L. F., Bookstein, F. L., Reddy, D. P. & Delson, E. Cranial allometry, phylogeography, and systematics of large-bodied papionins (primates: Cercopithecinae) inferred from geometric morphometric analysis of landmark data. Anat. Rec. A 275A , 1048–1072 (2003).
Cardini, A. & Elton, S. Is there a Wainer’s rule? Testing which sex varies most as an example analysis using GueSDat, the free Guenon Skull Database. Hystrix Ital. J. Mammal. 28 , 147–156 (2017).
Alemseged, Z. et al. Fossils from Mille-Logya, Afar, Ethiopia, elucidate the link between Pliocene environmental changes and Homo origins. Nat. Commun. 11 , 2480 (2020).
Robinson, J. R., Rowan, J., Campisano, C. J., Wynn, J. G. & Reed, K. E. Late Pliocene environmental change during the transition from Australopithecus to Homo . Nat. Ecol. Evol. 1 , 0159 (2017).
DiMaggio, E. N. et al. Late Pliocene fossiliferous sedimentary record and the environmental context of early Homo from Afar, Ethiopia. Science 347 , 1355–1359 (2015).
Su, D. F. & Harrison, T. The paleoecology of the Upper Laetolil Beds, Laetoli Tanzania: a review and synthesis. J. Afr. Earth Sci. 101 , 405–419 (2015).
White, T. D. et al. Macrovertebrate paleontology and the Pliocene habitat of Ardipithecus ramidus . Science 326 , 67–93 (2009).
WoldeGabriel, G. et al. The geological, isotopic, botanical, invertebrate, and lower vertebrate surroundings of Ardipithecus ramidus . Science 326 , 65–65e5 (2009).
Cerling, T. E. et al. Comment on the paleoenvironment of Ardipithecus ramidus . Science 328 , 1105-d (2010).
Domínguez-Rodrigo, M. Is the ‘savanna hypothesis’ a dead concept for explaining the emergence of the earliest hominins? Curr. Anthropol. 55 , 59–81 (2014).
Behrensmeyer, A. K., Bobe, R. & Alemseged, Z. in Hominin Environments in the East African Pliocene: An Assessment of the Faunal Evidence (eds Bobe, R. et al.) 1–24 (Springer, 2007).
Levin, N. E. Environment and climate of early human evolution. Annu. Rev. Earth Planet. Sci. 43 , 405–429 (2015).
Timmermann, A. et al. Climate effects on archaic human habitats and species successions. Nature 604 , 495–501 (2022).
Mondanaro, A. et al. A major change in rate of climate niche envelope evolution during hominid history. iScience 23 , 101693 (2020).
Cardini, A., Dunn, J., O’Higgins, P. & Elton, S. Clines in Africa: does size vary in the same way among widespread sub-Saharan monkeys? J. Biogeogr. 40 , 370–381 (2013).
Frost, S. R. & Delson, E. Fossil Cercopithecidae from the Hadar Formation and surrounding areas of the Afar Depression, Ethiopia. J. Hum. Evol. 43 , 687–748 (2002).
Dunn, J., Cardini, A. & Elton, S. Biogeographic variation in the baboon: dissecting the cline. J. Anat. 223 , 337–352 (2013).
Cardini, A. & Elton, S. Variation in guenon skulls (I): species divergence, ecological and genetic differences. J. Hum. Evol. 54 , 615–637 (2008).
Joordens, J. C. A., Feibel, C. S., Vonhof, H. B., Schulp, A. S. & Kroon, D. Relevance of the eastern African coastal forest for early hominin biogeography. J. Hum. Evol. 131 , 176–202 (2019).
Brunet, M. et al. New material of the earliest hominid from the Upper Miocene of Chad. Nature 434 , 752–755 (2005).
Brunet, M. et al. Australopithecus bahrelghazali , une nouvelle espèce d’Hominidé ancien de la région de Koro Toro (Tchad). Comptes Rendus Acad Sci. Sér. 2 322 , 907–913 (1996).
Jolly, C. J. The Seed-Eaters: a new model of hominid differentiation based on a baboon analogy. Man 5 , 5–26 (1970).
Habermann, J. M. et al. Gorongosa by the sea: first Miocene fossil sites from the Urema Rift, central Mozambique, and their coastal paleoenvironmental and paleoecological contexts. Palaeogeogr. Palaeoclimatol. Palaeoecol. 514 , 723–738 (2019).
Bobe, R. et al. The first Miocene fossils from coastal woodlands in the southern East African Rift. iScience 26 , 107644 (2023).
The IUCN Red List of Threatened Species. Version 2022-2. IUCN http://www.iucnredlist.org/ (2022).
QGIS Development Team. QGIS Geographic Information System (QGIS Association, 2023).
Gorelick, N. et al. Google Earth Engine: planetary-scale geospatial analysis for everyone. Remote Sens. Environ. https://doi.org/10.1016/j.rse.2017.06.031 (2017).
Buchhorn, M. et al. Copernicus Global Land Service: Land Cover 100m: collection 3: epoch 2019: Globe. Zenodo https://doi.org/10.5281/zenodo.3939050 (2020).
Hijmans, R. J., Cameron, S. E., Parra, J. L., Jones, P. G. & Jarvis, A. Very high resolution interpolated climate surfaces for global land areas. Int. J. Climatol. 25 , 1965–1978 (2005).
Mitteroecker, P. & Gunz, P. Advances in geometric morphometrics. Evol. Biol. 36 , 235–247 (2009).
Baken, E. K., Collyer, M. L., Kaliontzopoulou, A. & Adams, D. C. geomorph v4.0 and gmShiny: enhanced analytics and a new graphical interface for a comprehensive morphometric experience. Methods Ecol. Evol. 12 , 2355–2363 (2021).
Adams, D. C., Collyer, M. L., Kaliontzopoulou, A. & Baken, E. K. Geomorph: Software for Geometric Morphometric Analyses. R Package Version 4.0.4 (R Foundation for Statistical Computing, 2022).
R Development Core Team. R: A Language and Environment for Statistical Computing (R Foundation for Statistical Computing, 2015).
Guillerme, T., Puttick, M. N., Marcy, A. E. & Weisbecker, V. Shifting spaces: which disparity or dissimilarity measurement best summarize occupancy in multidimensional spaces? Ecol. Evol. 10 , 7261–7275 (2020).
Habel, K., Grasman, R., Gramacy, R. B., Mozharovskyi, P. & Sterratt, D. C. Geometry: Mesh Generation and Surface Tessellation (R Foundation for Statistical Computing, 2023).
Foote, M. Rarefaction analysis of morphological and taxonomic diversity. Paleobiology 18 , 1–16 (1992).
Download references
Acknowledgements
Special thanks to A. Cardini, S. Elton and S. Frost for generously providing access to datasets and providing spatial coordinates. We gratefully acknowledge the financial support of the Center for the Advanced Study of Human Paleobiology at GWU, the GWU Department of Anthropology and the GWU Office of the Provost. Thanks to members of the PAPER discussion group for fruitful discussion, to S. McPherron and S. Elton for helpful feedback after a conference presentation of some of the ideas in this paper, and to C. Campisano for answering our geological questions about the rift.
Author information
Authors and affiliations.
Department of Anthropology and Center for the Advanced Study of Human Paleobiology, The George Washington University, Washington DC, USA
W. Andrew Barr & Bernard Wood
You can also search for this author in PubMed Google Scholar
Contributions
W.A.B. devised the research question, compiled the datasets, wrote all code, interpreted all statistical analyses, wrote the first draft of the paper and revised the paper. B.W. contributed to the development of the research question, consulted on analytical strategy and revised the paper.
Corresponding author
Correspondence to W. Andrew Barr .
Ethics declarations
Competing interests.
The authors declare no competing interests.
Peer review
Peer review information.
Nature Ecology & Evolution thanks Jose Joordens and the other, anonymous, reviewer(s) for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Supplementary information.
Supplementary Figs. 1–3 and Tables 1–3.
Reporting Summary
Supplementary video 1.
A GIF animation showing the placement of random sampling units on the continent of Africa.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Reprints and permissions
About this article
Cite this article.
Barr, W.A., Wood, B. Spatial sampling bias influences our understanding of early hominin evolution in eastern Africa. Nat Ecol Evol (2024). https://doi.org/10.1038/s41559-024-02522-5
Download citation
Received : 18 February 2024
Accepted : 23 July 2024
Published : 20 August 2024
DOI : https://doi.org/10.1038/s41559-024-02522-5
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies
Sign up for the Nature Briefing newsletter — what matters in science, free to your inbox daily.

Disclaimer: Early release articles are not considered as final versions. Any changes will be reflected in the online version in the month the article is officially released.
Volume 30, Number 10—October 2024
One Health Investigation into Mpox and Pets, United States
Suggested citation for this article
Monkeypox virus (MPXV) is zoonotic and capable of infecting many mammal species. However, whether common companion animals are susceptible to MPXV infection is unclear. During July 2022–March 2023, we collected animal and environmental swab samples within homes of confirmed human mpox case-patients and tested for MPXV and human DNA by PCR. We also used ELISA for orthopoxvirus antibody detection. Overall, 12% (22/191) of animal and 25% (14/56) of environmental swab samples from 4 households, including samples from 4 dogs and 1 cat, were positive for MPXV DNA, but we did not detect viable MPXV or orthopoxvirus antibodies. Among MPXV PCR-positive swab samples, 82% from animals and 93% the environment amplified human DNA with a statistically significant correlation in observed cycle threshold values. Our findings demonstrate likely DNA contamination from the human mpox cases. Despite the high likelihood for exposure, however, we found no indications that companion animals were infected with MPXV.
Before 2022, the primary mode for monkeypox virus (MPXV) transmission was known to be zoonotic, and only limited human-to-human transmission was documented ( 1 , 2 ). Human MPXV infections resulting in mpox disease were hypothesized to be the result of direct or potentially indirect contact with infected wild mammals in Central and Western Africa ( 3 , 4 ). Our understanding of the potential for human-to-human spread of MPXV considerably broadened in the spring of 2022 ( 5 , 6 ). During that time, variant of clade II MPXV (clade IIb) was found in to be transmitted via direct contact among human populations and spreading primarily through sexual networks outside of mpox endemic regions ( 5 , 6 ).
Given the zoonotic origin and reported broad host-range of MPXV, efforts to understand and limit potential human-to-animal transmission are ongoing ( 4 , 7 ). The Centers for Disease Control and Prevention (CDC) provides guidance that persons with mpox stop or avoid contact with animals and that animals should be kept away from potentially infectious lesion material, objects, or surfaces ( 8 ). Mpox patients are generally urged by public health agencies to isolate at home unless hospitalization is clinically necessary ( 9 , 10 ). A person with mpox is considered infectious throughout their illness and until lesions have fully healed with new skin underneath; therefore, public health officials recommend that mpox patients isolating at home take proper infection control measures to prevent spread of infectious particles throughout the home ( 11 – 13 ). Unless infected persons take measures to completely isolate or reduce transmission potential, companion animals in close contact with mpox patients and their environments could be at higher risk for MPXV exposure than other mammal species, warranting special concern and investigation.
As of July 2024, no cases of MPXV infection or mpox disease had been confirmed in common domestic animals, such as dogs and cats, during the current global outbreak or any past outbreaks. One study in July 2022 described a 4-year-old dog in France that had been living and co-sleeping with 2 mpox case-patients ( 14 ). In that study, MPXV DNA was identified in swab samples from the dog’s skin and surface of mucosal lesions and in anal and oral swab samples ( 14 ). However, follow-up investigations suggested that the animal was not infected with MPXV ( 15 ). A similar case was documented in Brazil in August 2022, when a 5-month-old dog had lesions that were MPXV-positive by quantitative PCR ( 16 ). Whether viral DNA detection was a result of MPXV infection in those animals or the result of environmental contamination due to close contact with infected humans is unclear. We conducted a One Health investigation in the United States to assess the susceptibility of companion animals to mpox and the risk for reverse-zoonotic transmission within households.
Methods and Materials
Study population.
The CDC Muti-National Mpox Response’s One Health Team worked in collaboration with state and local jurisdictions to investigate the susceptibility of companion animals to MPXV infection. As part of that effort, CDC and state public health investigators collected blood samples from companion animals and swab specimens from companion animals and animal-associated objects. CDC tested swab and serum specimens via real-time PCR, orthopoxvirus (OPXV) serology, and viral culture. All animals tested were companion animals in a residence of a person with probable or confirmed mpox while the person was infectious. Animal sampling occurred within 21 days of any direct contact with the ill person before the person recovered ( Table 1 ).
During July 2022–March 2023, we conducted sample collection in the District of Columbia, Virginia, Minnesota, and Tennessee, USA. After the initial sampling timepoint, we attempted follow-up sampling from all households 3–4 months later to collect animal serum samples and assess postexposure or postinfection immune responses.
Questionnaire and Consent
State and local public health personnel from the District of Columbia, Virginia, Minnesota, and Tennessee assisted with the study by interviewing mpox cases in their jurisdictions and requesting their voluntary participation in the study. After a person gave verbal consent to participate, they were provided with a survey questionnaire and consent forms. The questionnaire ascertained details and a timeline of the human case, the animal’s health condition, general household information, types of contact between the person with mpox and the animal or animals in the household, and information about wild or domestic animals in and around the household. This project was reviewed by CDC clearance, cleared for human subjects, and determined to be nonresearch public health surveillance that did not require submission to the CDC institutional review board (project no. 0900f3eb81f79d72).
Swab Sample Collection
We performed all animal handling and sampling procedures in accordance with the approved CDC Institutional Animal Care Use Committee protocol (no. DOTMULX3183), in collaboration with state public health agencies, and with written consent of the animal’s owner. We collected a standardized set of polyester swab (Puritan, https://www.puritanmedproducts.com ) samples from the animal’s dorsum fur, ventral abdomen, oral cavity, and anorectal area under supervision of the owner. We sampled animal lesions, if present. We also collected animal-associated environmental (AAE) specimens from objects and surfaces often used by the animal.
Sample Processing and PCR
We processed swab samples by using the swab extraction tube system (SETS; Roche, https://www.roche.com ) with 400 μL of phosphate-buffered saline; after DNA extraction, we tested all samples for MPXV DNA by real-time PCR using an MPXV clade II–specific assay ( 17 ). In addition, we tested samples for human DNA by using the RNase-P PCR assay, which is used as an endogenous control when testing human specimens ( 18 ). We calculated Pearson correlation coefficients to assess the relationship between cycle threshold (Ct) values of MPXV clade II PCR–positive (Ct values < 37) and RNase-P reactive (Ct values <40) samples.
Viral Culture
We tested all PCR-positive swab samples for viable virus via cell culture by adding an aliquot of swab eluate to BSC-40 cell monolayers in T-25 flasks. We used an inoculation volume of 50 μL + 25 μL, depending on available eluate volume. We incubated flasks at 35.5°C in an atmosphere of 6% CO 2 in Roswell Park Memorial Institute medium ( 19 ). We incubated and observed flasks < 14 days or until ≈100% of monolayer showed cytopathic effect, following methods and media supplements described previously ( 11 ). To control the overgrowth of bacteria or fungi in T-25 flasks, we added penicillin/streptomycin, amphotericin B, and gentamicin to the cell culture medium. If we detected any bacterial or fungal contamination, we performed 4 cycles of medium replacement to wash the monolayers and repeated this process as needed to prevent overgrowth.
Blood Collection and Serologic Testing
We attempted blood collection from all cooperative animals for which the owner provided consent. We collected < 3 mL of blood from 20/34 animals during initial sampling and 21/25 animals during follow-up sampling. We cleaned the external venipuncture site with 90% ethanol and used a syringe or vacutainer needle for blood collection. For dogs and 1 rabbit, we collected blood via the cephalic or lateral saphenous veins. For cats, we collected blood via the jugular or medial saphenous veins. We stored and transported blood tubes at 4°C–20°C before centrifugation, after which we transferred serum into 2-mL cryotubes and stored at temperatures of at least –20°C until laboratory testing. We conducted a modified ELISA on all serum samples to determine presence of OPXV IgG antibodies, as previously described ( 20 , 21 ). We tested serum samples at a dilution of 1:100 by using microtiter plates coated with purified vaccinia virus (Dryvax strain) and using the A/G protein as the secondary antibody at a 1:10,000 concentration and developed plates for 25 minutes.
Data Analysis
When referring to animal swab samples, we defined prevalence as the proportion of total swabs collected from each animal from which we detected either MPXV DNA or RNase-P (RNP) by PCR. When referring to AAE samples, we defined prevalence as the proportion of total swabs collected from the AAE samples within that animal’s household that were MPXV-positive or RNP-positive. We also referred to detection of RNase-P via PCR as presence of human DNA.
For each animal, we calculated the duration of exposure, defined as cumulative number of days before sampling that an infectious owner had direct contact with the animal, including durations where direct contact was not reported but the animal was still sharing a common space with a person with mpox. Duration of exposure represented the total period that infectious lesion material (crusts or exudates) or other infectious particles were potentially shed or transferred within the home, to which the animal potentially had contact, either directly or via fomites.
We investigated factors reported in questionnaires that could affect animal MPXV exposure ( Table 1 ). Those factors included whether the owner was symptomatic during time of sampling (coded SXDS); the degree of animal outdoor activity (coded AOA), which we stratified by none (no outdoor activity), walks (periodic or frequent supervised walks outside), and yard (allowed in yard or outside unsupervised frequently or for prolonged periods); co-sleeping with the animal while the owner was infectious (coded CSI); and a score comprised of the sum of all reported interaction types between animals and humans that involved direct contact (coded DIS), which included cuddling, hugging, petting, kissing, co-sleeping, sharing food, and grooming ( Table 1 ).
We compared bivariate correlation coefficients among variables compiled from questionnaire data or diagnostic testing. We used SPSS Statistics 27 (IBM, https://www.ibm.com ) to compute Pearson correlation coefficients. We performed 2-tailed tests of significance and considered p values of < 0.05 or < 0.01 statistically significant, as applicable.
Overall, we sampled 34 individual companion animals from 21 households: 24 domestic dogs, 9 domestic cats, and 1 domestic rabbit ( Table 2 ). The age of the animals ranged from 4 months to 16 years; 22 were male and 12 were female. All but 1 household had a single human mpox case; the other household had 2 cases. We collected a total of 191 swab specimens from animals and 56 AAE specimens. If excess blood was available, we opportunistically tested select blood specimens via PCR, including 10 whole blood specimens preserved in EDTA and 1 blood clot. At examination, we observed skin lesions in 6 dogs and 1 cat, and lesion features and locations varied.
PCR for Animal Samples
Samples collected from 5 individual animals (4 dogs, 1 cat) from 4 households were MPXV-positive; 2 of the dogs shared a household. Total animal swab MPXV positivity was 12% (22/191); 21 MPXV-positive swabs were from dogs, and 1 was from a cat ( Table 3 ). All MPXV-positive animals also had > 1 sample with an RNP-positive test result. Ct values of MPXV-positive samples were 25.2–36.7 (mean 34.5). Results of specific sample types collected were 29% (4/14) for skin lesions, 16% (6/37) for ventral skin or fur, 12% (4/33) for dorsal fur, 11% (4/35) for periocular area, 8% (3/36) for anorectal area, and 3% (1/36) for oral.
Among animal MPXV-positive specimens, 82% were RNP-positive, whereas 25% of the MPXV DNA–negative specimens were RNP-positive ( Table 3 ). Ct values of MPXV-positive specimens that were RNP-positive positively correlated (p<0.01). In animal specimens, 18% (4/22) were MPXV-positive and RNP-negative, and positive Ct values (range 35.3–36.1) were near the upper limit of detection (Ct 37) for the assay. We did not detect MPXV DNA in any of the blood specimens tested via MPXV PCR. In addition, MPXV DNA prevalence in animal samples alone and when combined with AAE specimens significantly correlated with RNP prevalence in those same samples (p<0.05).
We collected AAE specimens from 20/21 households, predominately from animal beds or bedding, toys, and food and water dishes. Among households, 29% (6/21) were positive for MPXV DNA, as were 25% (14/56) of collected specimens, 93% (13/14) of which were positive for MPXV and RNP ( Table 3 ). In those same samples, AAE MPXV DNA prevalence positively correlated with human DNA prevalence (p<0.05). Of the 4 households with MPXV-positive animal swab specimens, all had MPXV-positive AAE swabs with Ct values of 29.9–35.9 (mean 32.8). For AAE specimens that were MPXV- and RNP-positive, the MPXV and RNase-P Ct values were significantly correlated (p<0.01). Of all AAE specimens, 66% (37/56) were RNP-positive, of which 82% (9/11) of specimens with Ct values <37 were in the 4 households with MPXV-positive AAE and animal swab samples.
Viral Culture and Serology
We attempted viral culture from all specimens with Ct values < 36 (n = 31), and all were negative with no signs of cytopathic effect. Three specimens from 2 dogs had bacterial contamination causing destruction of monolayer by day 6 or 7 postinfection, despite mitigating steps or retesting, and the harvested culture media tested negative by MPXV-specific PCR. In addition, all initial (n = 20) and follow-up (n = 22) serum specimens collected were ELISA-negative, and we detected no OPXV IgG. For 1 dog that had samples with the lowest MPXV Ct values, we collected 2 follow-up samples 2 months apart. Of the 5 animals that had MPXV-positive swab specimens, 3 did not have blood sampled at the initial timepoint due to noncompliance or aggression, and 3 were not available at the postexposure sampling timepoint.
Questionnaire Analysis
In total, 32% (11/34) of animals had preexisting health issues and 5 animals had preexisting skin lesions. In addition to the 5 animals with skin lesions that developed before owner symptom onset (all sampled), 2 additional animals had lesions that developed after owner symptom onset. We observed and sampled those lesions during the initial sampling visit, and 1 animal had skin and fur, periocular, and anorectal specimens that were PCR-positive for MPXV DNA, but we did not detect MPXV DNA from the lesion specimen, and serology results also were negative.
In total, 33% (7/21) of households reported no contact change with their animals. Reported types of changes in animal interactions included reducing frequency of interactions (9/21), stopping interactions (8/21), use of PPE during interactions (6/21), and relocating or isolating the animal (4/21); 1 household reported relegating animal care to uninfected persons outside the household. However, all but 1 household reported > 1 type of direct contact activity with each animal after the MPXV-positive human in the household had symptoms develop ( Table 1 ).
Households comprised apartments (n = 11) or single-family homes (n = 10), and approximate size range was 500–3,500 ft 2 ( Table 1 ). We observed a significant negative correlation between household size and prevalence of either MPXV (p<0.05) or human DNA (p<0.01) in animal samples and human DNA prevalence in environmental samples (p<0.01). Apart from human DNA prevalence, household size, and environmental MPXV prevalence, we observed no other statistically significant relationships for other variables potentially influencing prevalence of MPXV DNA in animal samples.
CDC advises that persons with mpox should avoid contact with animals, including pets, until lesions have fully healed to prevent potential virus spillback. That recommendation is because of uncertainty regarding susceptibility of companion animals to MPXV ( 9 ). If MPXV-infected persons cannot avoid contact with pets within the household, practicing appropriate infection control will prevent further exposure potential. In most households we visited, recommended quarantine and infection control procedures were not consistently followed.
Despite MPXV-positive swab specimens detected on the skin or fur of dogs and cats and in associated environmental samples, no dogs or cats with live virus or antibodies detected have been reported globally. In 2 cases outside of the United States in which MPXV DNA was detected in dogs ( 14 , 16 ), apart from apparent skin lesions, no other signs of infection were reported in the animals, including virus cultured from samples or OPXV antibodies detected by serology after additional investigation ( 15 ).
In our household study, skin lesions in 7 animals were the only observable clinical features that were potentially consistent with mpox disease. However, 5 animals exhibited lesions before owner symptom onset, and the 2 animals with skin lesions that were observed after owner symptom onset were negative for MPXV by PCR. Only 1 animal had MPXV-positive lesions sampled, a dog with lesion swab samples collected from a grouping of 3 large lesions on its rear leg, and the average Ct value of samples was 25.2. After further testing to consider potential DNA contamination from the owner, that sample also had the lowest average RNase-P Ct value (29.3) of all samples tested. In addition, that dog’s lesions were reported to have formed before symptom onset in the owner, culture attempts from that and all other samples were negative, and OPXV antibodies were not detected during any timepoint tested. Therefore, after reviewing all the data, we did not consider this animal a confirmed mpox case.
All animals with MPXV-positive samples in this study also had RNP-positive specimens collected, indicating the presence of human DNA. The statistically significant correlation of MPXV- and RNP-positive samples, MPXV PCR results showing high Ct values indicating low viral DNA loads, and the lack of viable virus or antibodies in the collected samples strongly suggest that observed lesions or scabs in these animals were not the result of MPXV infection. In addition, from our knowledge of MPXV pathology, an MPXV lesion would most likely produce high viral loads and at levels higher than for other sample types ( 22 ).
As reported in other household environmental sampling studies, MPXV DNA can be widely detected in indoor or household settings ( 11 , 12 , 23 – 25 ). In this study, we found that households with smaller shared spaces were significantly correlated with both MPXV and human DNA prevalence, suggesting that the risk for MPXV exposure could be higher in smaller living quarters. Given the capability of MPXV DNA to disseminate within the household of a person with mpox, and after consideration of the PCR results detailed here, persons with mpox, not the companion animals, likely were the source of the MPXV DNA we detected in the household.
The potential for contamination from either direct contact with a person with mpox or indirect exposure to materials containing MPXV DNA should be considered when interpreting results of PCR testing from companion animals. In addition, case definitions should consider potential extraneous contamination and require more than a PCR-positive result from an animal to be considered a confirmed animal mpox case ( 26 ). Contamination should also be considered as a reason for a positive PCR result and false positive results in humans with nonspecific lesions who have potentially had contact with an mpox case-patient.
MPXV infection in companion animals, if they are suitable hosts, is uncharacterized; clinical signs, viral shedding, and duration of infectious period are unknown. Thus, although unlikely, given the limits of our sampling design, it is possible that an infected animal escaped detection in our study. However, the overall PCR and serologic evidence best fits the hypothesis that the MPXV DNA detected in animal samples submitted for PCR testing is a result of DNA contamination from the infected human within the household.
More work is needed to determine the susceptibility of companion animals to clade-IIb MPXV. Thus, CDC still recommends that companion animal owners with mpox limit their interactions with their pets while infectious, particularly if they are sharing smaller living spaces. That precautionary measure is recommended until more information is available about the susceptibility of common mammalian companion animal species to mpox.
In conclusion, no strong evidence yet exists to suggest that common companion animals, such as dogs or cats, are susceptible to infection with clade IIb MPXV. Given high likelihood for exposure among most of these animals, the paucity of evidence indicating infection might indicate resistance to infection. Nonetheless, to prevent further viral spread and potential evolution and establishment of new endemic areas, during public health emergencies caused by emerging zoonotic diseases, responders should apply a One Health approach to investigate potential spillback of human infections to animals, including pets.
Mr. Morgan is a biologist in the Poxvirus and Rabies Branch, Division of High Consequence Pathogens and Pathology, National Center for Emerging and Zoonotic Infectious Diseases, Centers for Disease Control and Prevention. His research interests include the virus-host interactions of orthopoxviruses and lyssaviruses in the environment.
Acknowledgments
The authors thank the Epidemiology, Laboratory and Testing, and STLT (State, Tribal, Local, or Territorial) Task Forces of the CDC 2022 Multinational Mpox Response and the CDC Poxvirus and Rabies Branch, Division of High Consequence Pathogens and Pathology, National Center for Emerging and Zoonotic Infectious Diseases. We also acknowledge additional persons and entities who assisted with this study, including the Minnesota Department of Health, including Patrice Vandelinde, Victoria Lappi, and Anna Strain; the Virginia Department of Health, including Kenneth Gordon, Christina Chommanard, Luisa Angel Cortes, Clarissa Bonnefond, Lisa Engle, and Cynthia Rieken; the Tennessee Department of Health and Agriculture, including Jane Yackley, Dilani Goonewardene, and Whitnie Smartt; and DC Department of Health, including Sarah Gillani, Will Still, and Karla Miletti. In addition, we acknowledge, Casey Barton-Behravesh, Yoshinori Nakazawa, Modupe Osinubi, Ashutosh Wadhwa, and Ariel Caudle for their assistance.
All funding for this study was provided by the Centers for Disease Control and Prevention’s 2022 Multinational Mpox Response (CDC Mpox Response). The CDC Mpox Response provided technical review and oversight of this manuscript before publication. This study and report were also supported in part by an appointment to the Applied Epidemiology Fellowship Program, administered by the Council of State and Territorial Epidemiologists (CSTE) and funded by the Centers for Disease Control and Prevention (CDC) (cooperative agreement no. 1NU38OT000297-03-00).
- Nolen LD , Osadebe L , Katomba J , Likofata J , Mukadi D , Monroe B , et al. Extended human-to-human transmission during a monkeypox outbreak in the Democratic Republic of the Congo. Emerg Infect Dis . 2016 ; 22 : 1014 – 21 . DOI PubMed Google Scholar
- Durski KN , McCollum AM , Nakazawa Y , Petersen BW , Reynolds MG , Briand S , et al. Emergence of Monkeypox - West and Central Africa, 1970-2017. MMWR Morb Mortal Wkly Rep . 2018 ; 67 : 306 – 10 . DOI PubMed Google Scholar
- Reynolds MG , Doty JB , McCollum AM , Olson VA , Nakazawa Y . Monkeypox re-emergence in Africa: a call to expand the concept and practice of One Health. Expert Rev Anti Infect Ther . 2019 ; 17 : 129 – 39 . DOI PubMed Google Scholar
- Reynolds MG , Guagliardo SAJ , Nakazawa YJ , Doty JB , Mauldin MR . Understanding orthopoxvirus host range and evolution: from the enigmatic to the usual suspects. Curr Opin Virol . 2018 ; 28 : 108 – 15 . DOI PubMed Google Scholar
- Sah R , Abdelaal A , Reda A , Katamesh BE , Manirambona E , Abdelmonem H , et al. Monkeypox and its possible sexual transmission: where are we now with its evidence? Pathogens . 2022 ; 11 : 924 . DOI PubMed Google Scholar
- Low N , Bachmann LH , Ogoina D , McDonald R , Ipekci AM , Quilter LAS , et al. Mpox virus and transmission through sexual contact: Defining the research agenda. PLoS Med . 2023 ; 20 : e1004163 . DOI PubMed Google Scholar
- McQuiston JH , Braden CR , Bowen MD , McCollum AM , McDonald R , Carnes N , et al. The CDC domestic mpox response—United States, 2022–2023. MMWR Morb Mortal Wkly Rep . 2023 ; 72 : 547 – 52 . DOI PubMed Google Scholar
- Centers for Disease Control and Prevention . Mpox in the home [ cited 2023 Dec 8 ]. https://www.cdc.gov/poxvirus/mpox/veterinarian/mpox-in-animals.html
- Adler H , Gould S , Hine P , Snell LB , Wong W , Houlihan CF , et al. ; NHS England High Consequence Infectious Diseases (Airborne) Network . Clinical features and management of human monkeypox: a retrospective observational study in the UK. Lancet Infect Dis . 2022 ; 22 : 1153 – 62 . DOI PubMed Google Scholar
- Minhaj FS , Ogale YP , Whitehill F , Schultz J , Foote M , Davidson W , et al. ; Monkeypox Response Team 2022 . Monkeypox Response Team 2022. Monkeypox outbreak—nine states, May 2022. MMWR Morb Mortal Wkly Rep . 2022 ; 71 : 764 – 9 . DOI PubMed Google Scholar
- Morgan CN , Whitehill F , Doty JB , Schulte J , Matheny A , Stringer J , et al. Environmental persistence of monkeypox virus on surfaces in household of person with travel-associated infection, Dallas, Texas, USA, 2021. Emerg Infect Dis . 2022 ; 28 : 1982 – 9 . DOI PubMed Google Scholar
- Pfeiffer JA , Collingwood A , Rider LE , Minhaj FS , Matheny AM , Kling C , et al. High-contact object and surface contamination in a household of persons with monkeypox virus infection—Utah, June 2022. MMWR Morb Mortal Wkly Rep . 2022 ; 71 : 1092 – 4 . DOI PubMed Google Scholar
- Centers for Disease Control and Prevention . Mpox: isolation and infection control at home [ cited 2023 Jan 21 ]. https://www.cdc.gov/poxvirus/monkeypox/clinicians/infection-control-home.html
- Seang S , Burrel S , Todesco E , Leducq V , Monsel G , Le Pluart D , et al. Evidence of human-to-dog transmission of monkeypox virus. Lancet . 2022 ; 400 : 658 – 9 . DOI PubMed Google Scholar
- The French Agency for Food . Monkeypox: what is the risk of spreading to pets? [in French] [ cited 2022 Dec 16 ]. https://www.anses.fr/fr/content/variole-du-singe-quel-risque-de-diffusion-aux-animaux-de-compagnie
- Brazilian Ministry of Health . Ministry of Health is notified of the first case of monkeypox in a domestic animal [in Portuguese] [ cited 2022 Dec 3 ]. https://www.gov.br/saude/pt-br/assuntos/noticias/2022/agosto/ministerio-da-saude-e-notificado-do-primeiro-caso-de-variola-dos-macacos-em-animal
- Li Y , Zhao H , Wilkins K , Hughes C , Damon IK . Real-time PCR assays for the specific detection of monkeypox virus West African and Congo Basin strain DNA. J Virol Methods . 2010 ; 169 : 223 – 7 . DOI PubMed Google Scholar
- Centers for Disease Control and Prevention . Test procedure: monkeypox virus generic real-time PCR test [ cited 2023 Oct 7 ]. https://www.cdc.gov/poxvirus/mpox/pdf/PCR-Diagnostic-Protocol-508.pdf
- Hughes CM , Liu L , Davidson WB , Radford KW , Wilkins K , Monroe B , et al. A tale of two viruses: coinfections of monkeypox and varicella zoster virus in the Democratic Republic of Congo. Am J Trop Med Hyg . 2020 ; 104 : 604 – 11 . DOI PubMed Google Scholar
- Karem KL , Reynolds M , Braden Z , Lou G , Bernard N , Patton J , et al. characterization of acute-phase humoral immunity to monkeypox: use of immunoglobulin M enzyme-linked immunosorbent assay for detection of monkeypox infection during the 2003 North American outbreak. Clin Diagn Lab Immunol . 2005 ; 12 : 867 – 72 . PubMed Google Scholar
- Hutson CL , Olson VA , Carroll DS , Abel JA , Hughes CM , Braden ZH , et al. A prairie dog animal model of systemic orthopoxvirus disease using West African and Congo Basin strains of monkeypox virus. J Gen Virol . 2009 ; 90 : 323 – 33 . DOI PubMed Google Scholar
- Kim H , Kwon R , Lee H , Lee SW , Rahmati M , Koyanagi A , et al. Viral load dynamics and shedding kinetics of mpox infection: a systematic review and meta-analysis. J Travel Med . 2023 ; 30 : taad111 . DOI PubMed Google Scholar
- Gould S , Atkinson B , Onianwa O , Spencer A , Furneaux J , Grieves J , et al. ; NHS England Airborne High Consequence Infectious Diseases Network . Air and surface sampling for monkeypox virus in a UK hospital: an observational study. Lancet Microbe . 2022 ; 3 : e904 – 11 . DOI PubMed Google Scholar
- Nörz D , Pfefferle S , Brehm TT , Franke G , Grewe I , Knobling B , et al. Evidence of surface contamination in hospital rooms occupied by patients infected with monkeypox, Germany, June 2022. Euro Surveill . 2022 ; 27 : 2200477 . DOI PubMed Google Scholar
- Atkinson B , Burton C , Pottage T , Thompson K-A , Ngabo D , Crook A , et al. Infection-competent monkeypox virus contamination identified in domestic settings following an imported case of monkeypox into the UK. Environ Microbiol . 2022 ; 24 : 4561 – 9 . DOI PubMed Google Scholar
- Centers for Disease Control and Prevention . Interim CDC case definition for animal cases of monkeypox [ cited 2023 Mar 14 ]. https://www.cdc.gov/poxvirus/mpox/veterinarian/animal-officials.html#case-def
- Table 1 . Summary of variables coded from household and questionnaire data used in a One Health investigation into mpox and pets, United States
- Table 2 . Animal and environment sampling and diagnostic testing data from a One Health investigation into mpox and pets, United States
- Table 3 . PCR results of for monkeypox virus clade II and RNase-P DNA assays from swab samples of companion animals and animal-associated objects and surfaces during a One Health investigation into mpox...
Suggested citation for this article : Morgan CN, Wendling NM, Baird N, Kling C, Lopez L, Navarra T, et al. One Health investigation into mpox and pets, United States. Emerg Infect Dis. 2024 Oct [ date cited ]. https://doi.org/10.3201/eid3010.240632
DOI: 10.3201/eid3010.240632
Original Publication Date: August 14, 2024
Table of Contents – Volume 30, Number 10—October 2024
| EID Search Options |
|---|
| – Search articles by author and/or keyword. |
| – Search articles by the topic country. |
| – Search articles by article type and issue. |
Please use the form below to submit correspondence to the authors or contact them at the following address:
Jeffrey B. Doty, Centers for Disease Control and Prevention, 4055 Tudor Center Dr, Anchorage, Alaska 99508, USA
Comment submitted successfully, thank you for your feedback.
There was an unexpected error. Message not sent.
Metric Details
Article views: 836.
Data is collected weekly and does not include downloads and attachments. View data is from .
What is the Altmetric Attention Score?
The Altmetric Attention Score for a research output provides an indicator of the amount of attention that it has received. The score is derived from an automated algorithm, and represents a weighted count of the amount of attention Altmetric picked up for a research output.
IMAGES
COMMENTS
The typical research paper is a highly codified rhetorical form [1, 2]. Knowledge of the rules—some explicit, others implied—goes a long way toward writing a paper that will get accepted in a peer-reviewed journal. Primacy of the research question. A good research paper addresses a specific research question.
Set the top, bottom, and side margins of your paper at 1 inch. Use double-spaced text throughout your paper. Use a standard font, such as Times New Roman or Arial, in a legible size (10- to 12-point). Use continuous pagination throughout the paper, including the title page and the references section.
The main guidelines for formatting a paper in APA Style are as follows: Use a standard font like 12 pt Times New Roman or 11 pt Arial. Set 1 inch page margins. Apply double line spacing. If submitting for publication, insert a APA running head on every page. Indent every new paragraph ½ inch.
Research paper format is an essential aspect of academic writing that plays a crucial role in the communication of research findings.The format of a research paper depends on various factors such as the discipline, style guide, and purpose of the research. It includes guidelines for the structure, citation style, referencing, and other elements of the paper that contribute to its overall ...
Indent new paragraphs 1/2 inch. Use a running head for each page in the upper right-hand corner, which consists of the paper's title in capital letters followed by the page number. The citations page at the end should be titled "References." In-text citations should include the publication date: (Smith, 1999, p. 50).
This article provides an overview of writing for publication in peer-reviewed journals. While the main focus is on writing a research article, it also provides guidance on factors influencing journal selection, including journal scope, intended audience for the findings, open access requirements, and journal citation metrics.
Develop a thesis statement. Create a research paper outline. Write a first draft of the research paper. Write the introduction. Write a compelling body of text. Write the conclusion. The second draft. The revision process. Research paper checklist.
Sections of an Original Research Article. Original research articles make up most of the peer-reviewed literature (), follow a standardized format, and are the focus of this article.The 4 main sections are the introduction, methods, results, and discussion, sometimes referred to by the initialism, IMRAD.
A complete research paper in APA style that is reporting on experimental research will typically contain a Title page, Abstract, Introduction, Methods, Results, Discussion, and References sections. 1 Many will also contain Figures and Tables and some will have an Appendix or Appendices. These sections are detailed as follows (for a more in ...
Communicating research findings is an essential step in the research process. Often, peer-reviewed journals are the forum for such communication, yet many researchers are never taught how to write a publishable scientific paper. In this article, we explain the basic structure of a scientific paper and describe the information that should be included in each section. We also identify common ...
Overall, while writing an article from scratch may appear a daunting task for many young researchers, the process can be largely facilitated by good groundwork when preparing your research project, and a systematic approach to the writing, following these simple guidelines for each section (see summary in Fig. 1). It is worth the effort of ...
Indent the first line of every paragraph of text 0.5 in. using the tab key or the paragraph-formatting function of your word-processing program. Page numbers: Put a page number in the top right corner of every page, including the title page or cover page, which is page 1. Student papers do not require a running head on any page.
For guidance, Nature 's standard figure sizes are 90 mm (single column) and 180 mm (double column) and the full depth of the page is 170 mm. Amino-acid sequences should be printed in Courier (or ...
Abstract. The purpose of your abstract is to express the key points of your research, clearly and concisely. An abstract must always be well considered, as it is the primary element of your work that readers will come across. An abstract should be a short paragraph (around 300 words) that summarizes the findings of your journal article.
Lewiston, ME. v. 10‐2014. This is a reference sheet to help you remember the common format we expect you to use on your formal lab write‐ups. Refer to the "How to Write Guide" for the details. Other than the title, use 12 point type, preferably Calibri, Times New Roman, or Courier.
How do you format a research paper? Learn more about the basic outline for any research paper, complete with example text and formatting tips.
Basic guidelines for formatting the reference list at the end of a standard APA research paper Author/Authors Rules for handling works by a single author or multiple authors that apply to all APA-style references in your reference list, regardless of the type of work (book, article, electronic resource, etc.) ...
3 or 4 data sets per figure; well-selected scales; appropriate axis label size; symbols clear to read; data sets easily distinguishable. Each photograph must have a scale marker of professional quality in a corner. Use color ONLY when necessary. Color must be visible and distinguishable when printed in black & white.
Research in the health sciences can be qualitative, quantitative, or a combination of the two. This guide will focus primarily on quantitative research. Quantitative research articles are usually written in a standardized format called the IMRaD format. This acronym refers to the Introduction, Methods, Results, (and) Discussion sections of the articles.. There is also usually a Conclusions secti
Other tips to help you with the Results section: . If you need to cite the number in the text (not just in the table), and the total in the group is less than 50, do not include percentage. Write "7 of 34," not "7 (21%).". . Do not forget, if you have multiple comparisons, you probably need adjustment.
Original Research: This is the most common type of journal manuscript used to publish full reports of data from research. It may be called an Original Article, Research Article, Research, or just Article, depending on the journal. The Original Research format is suitable for many different fields and different types of studies.
In this comprehensive guide, we'll explain the IMRAD format, why it's so important for research writing, and how to use it effectively. Follow along to learn the ins and outs of crafting papers in the gold-standard IMRAD structure. In this article, I'll walk you through the IMRAD format step-by-step. I'll explain each section, how to ...
As you research the answers to the topic questions. you can use the information two ways: 1. If it is from a non-com puter source, you can use. index cards to copy the information needed, or ca n ...
Assignment 1 - Outline Summary Value: 15% of the final grade. Due Date: on or before 11:55 p.m. AT on Sunday of Unit 2. Learning Objectives Critically review and evaluate quantitative research. Search for and explore peer-reviewed counselling quantitative research articles; synthesize and critique selected studies' findings. Demonstrate elementary research design skills.
The study was reviewed and approved by the institution's Undergraduate Research Ethics Committee. The sample size for the study was derived based on power calculation conducted using G*Power (Faul et al., 2007). Assuming a small-to-medium effect size, 80% power and an alpha level of 0.05, the calculation indicated that a sample size of 60 ...
Aim. The aim of this study, which forms part of a wider research [], is to analyse the changes in the experience, perception of cross-level clinical coordination of primary care (PC) and secondary care (SC) doctors and related factors in the Catalan health system between 2017 and 2022.Study design and areas of study. A comparative analysis was conducted of two cross-sectional studies based on ...
There is a pressing need for research on the geography of early hominin morphoclines to estimate how morphologically representative the hominin fossil sample from the eastern branch may be.
Disclaimer: Early release articles are not considered as final versions. Any changes will be reflected in the online version in the month the article is officially released. Volume 30, Number 10—October 2024 Research One Health Investigation into Mpox and Pets, United States